



IntelliPaper
Abstract
Rhabdomyomas are a rare and benign, slow growing tumour of the skeletal muscles. They are even further classified into cardiac and extracardiac types according to their location. Extracardiac rhabdomyomas can be further divided based on cellular differentiation, such as; fetal, genital, and adult subtype [1] . Adult Type Rhabdomyomas shown to have clinical predominance towards adult males and more commonly reported in the head and neck region as compared to other parts of the body. This type of benign tumour also has a high recurrence rate. In this case review we discuss a rare case of floor of mouth rhabdomyoma.
Explore Digital Article Text
I. INTRODUCTION
Rhabdomyomas are a rare and benign, slow growing tumour of the skeletal muscles. They are even further classified into cardiac and extracardiac types according to their location. Extracardiac rhabdomyomas can be further divided based on cellular differentiation, such as; fetal, genital, and adult subtype [1]. Adult Type Rhabdomyomas shown to have clinical predominance towards adult males and more commonly reported in the head and neck region as compared to other parts of the body. This type of benign tumour also has a high recurrence rate. In this case review we discuss a rare case of floor of mouth rhabdomyoma.
II. CASE REPORT
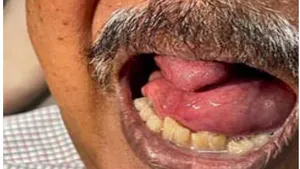
We present this case a 67-year-old gentleman with a recurrent swelling of the floor of mouth with intact mucosa. The swelling was gradually increasing in size over the past 3 years causing drooling of saliva and speech articulation disorder, but no interference with mastication and no difficulty in swallowing. Clinical examination revealed non-pulsatile, soft, non-cystic, smooth surface mucosa with noticeable elevation of floor of mouth. The mass was occupying the right floor of mouth extending to anterior two third of tongue and laterally over the left extending to posterior two third of tongue with no involvement of base of tongue.
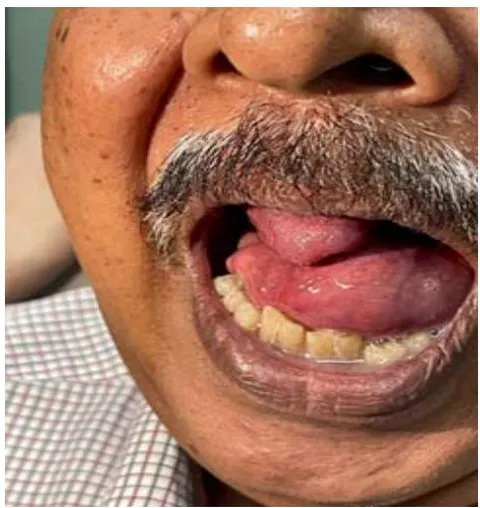
Figure 1

Figure 2
Figure 1 & 2: Demonstrates Patient's Presentation with a Floor of Mouth Mass
The patient was a referred case from another tertiary centre and at the time of consultation the patient has had a Computerized Tomography (CT) scan done. The images from the CT scan showed a lobulated enhancing floor of mouth mass with no bony involvement. A Magnetic Resonance Imaging (MRI) was then ordered for a precise evaluation of soft tissue and muscle involvement.
MRI rendered the mass as hyperintense on T1W/T2W measuring 6.3 x 4.6 x 7.3 (AP x W x CC) cm with involvement of lingula septum, bilateral sublingual glands, mylohyoid and genioglossus/geniohyoid complexes with elevation and posterior displacement of tongue causing narrowing oral cavity and oropharynx.
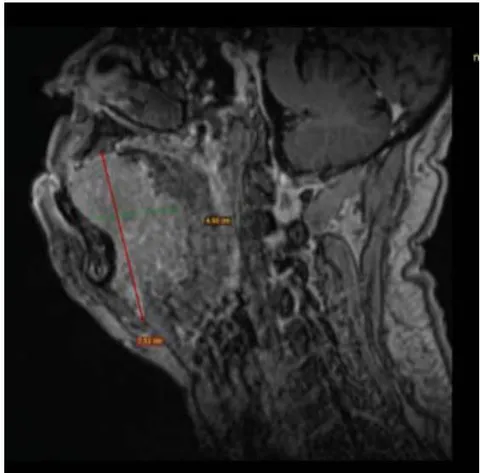
Figure 3
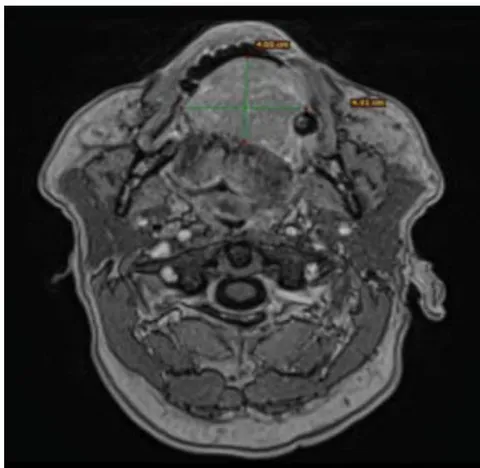
Figure 4
Figure 3 & 4: Figure 3 (Saggital View) and Figure 4 (Axial View) Demonstrates MRI Images at T1w/T2w
Patient then underwent a surgical excision of the mass via a combined transoral and transcervical approach. Intra-operative findings revealed a non-vascularized multilobulated mass originating from the submucosa of the floor of the mouth not involving the surrounding muscles. The mass was excised completely.

Figure 5: Illustrates the Intra-Operative Findings of the Tumour Itself
In the histopathological examination, the mass is described microscopically as benign circumscribed tissue composed of irregularly arranged sheets of large polyhedral cells separated by fibrovascular septa into lobules. The cells also display vesicular nuclei, mild nuclear pleomorphism, occasional prominent nucleoli, and very minimal evident of mitotic activity. Immunohistochemically, many of these cells possess intracytoplasmic glycogen and expresses desmin.
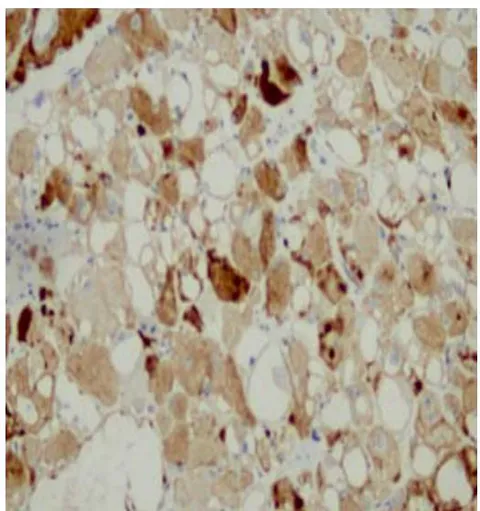
Figure 6
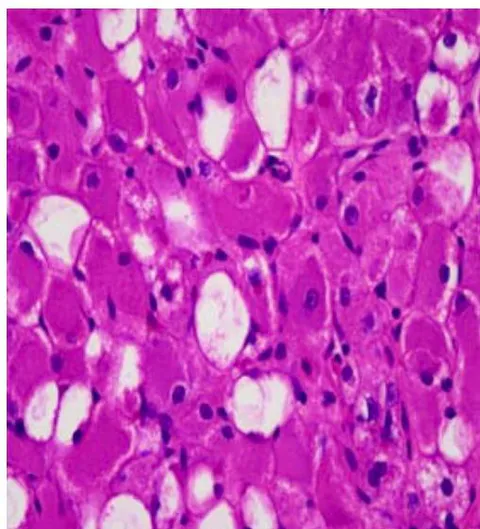
Figure 7
Figure 6 and 7 Illustrates Light Microscopy Images
Figure 6: Magnification 200x showed cells mostly stain positive towards Desmin and negative stain for S-100
Figure 7: Magnification 400x with Hematoxylin and Eosin stain; shows cells irregularly arranged. No necrosis observed
About half was stained positive for SMA, and of these cells are immunoreactive towards myogenin and KI-67. These cells were stained negative for calretinin, CD68, EMA, inhibin, MyoD1, NSE and S100. These are findings consistent with adult type rhabdomyoma.
III. DISCUSSION
Adult type extracardiac rhabdomyomas are rare, slow growing benign tumours which accounts less than of all skeletal muscle tumours. In spite of this rarity, it is most commonly reported in the head and neck region with a predominance seen among middle aged males irrespective of racial background[1]. Generally, Adult Type Rhabdomyoma are reported as solitary mass, however some literatures have documented rare cases of multilobulated lesions.
The symptoms of rhabdomyomas are a result of mass on the site and the size of tumour itself. Presenting complaints from patients is usually due to a mass effect of the tumour on the surrounding tissues, commonly dysphonia, dysphagia and sometimes airway compromise [1]. In view of the nature of it being a painless and slow growing tumour, patients tend to present clinically with already a significantly large mass and a history of subacute progression of symptoms [3].
Radiological imaging of choice for adult type rhabdomyomas are CT scans and MRI. Due to the rarity of extracardiac rhabdomyomas in the head and neck region, the appearance of this neoplasm is not very well described from radiological imaging in literatures. However, studies have shown these imaging are useful in determining the site, extent, appearance and the characteristic of the tumour. In a CT scan adult type rhabdomyoma may mimic a malignant lesion due to the indistinct borders between the tumour and adjacent structures. A MRI would aid in a better evaluation of the soft tissues. In contrast to malignant lesions, benign lesions do not show invasions into surrounding soft tissues.
Adult type Rhabdomyomas of the head and neck regions are treated with surgical excision of the tumour and regular surveillance follow-up. In a multilobulated tumour there is an incidence of recurrence up to of cases.
Histologically, the features of adult type rhabdomyomas are very characteristic. In the histopathologic staining these cells characteristically stain positive to myoglobin, desmin, MSA and stain negative to S100, distinguishing them from granular cell tumours and hibernoma [3]. Desmin being the most reliable marker as it is found in both primitive and mature cells expressing skeletal or smooth muscle differentiation [2].
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
Cite this article
Related Research

Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.


