



IntelliPaper
Abstract
Background: Multiple Myeloma, a haematological malignancy that is characterized by the clonal proliferation of plasma cells often presents with renal dysfunction, anaemia and bone lesions (CRAB criteria). Diagnosing Multiple Myeloma in patients who are suffering from preexisting chronic kidney disease and other comorbidities such as Diabetes and Hypertension can be quite challenging as these diseases have overlapping clinical presentation. This case serves to highlight the complexities in diagnosing MM in a patient with well-controlled comorbid diseases and atypical renal presentation.
The Case: We describe a case of a 66-year-old female patient with chronic kidney disease stage 2, diabetes mellitus type 2, chronic hypertension and coronary heart disease that presented to the clinic with complaints of lower limb oedema and severe proteinuria. Laboratory findings revealed a hypochromic normocytic anaemia and increased ESR. Initially, it was suspected to be diabetic nephropathy but the patient’s optimal glycaemic control as well as the disproportionate levels of anaemia and proteinuria cast doubts on that diagnosis. A sternal puncture was performed and revealed Multiple Myeloma.
Conclusion: Physicians must consider multiple myeloma as a part of a differential diagnosis in patients with chronic kidney disease presenting with atypical haematological or renal signs, particularly those that have a multitude of comorbidities. Such clinical suspicion may lead to early diagnosis, thus greatly reducing mortality rates in this patient category. This case also serves to highlight the importance of utilising a multidisciplinary approach in patients with overlapping comorbid conditions.
Explore Digital Article Text
I. INTRODUCTION
Multiple myeloma (MM) is a malignancy of haematological origin characterized by the clonal proliferation of cancerous plasma cells(1) in the bone marrow. MM is the second most-common haematological malignancy in adults and commonly presents in elderly patients over the age of 60(2). The precise aetiology of MM is unknown(3). This disease often presents with a constellation of symptoms and laboratory abnormalities, including anaemia, renal dysfunction, hypercalcemia, and bone lesions, collectively known as the CRAB criteria(4).
Diagnosing multiple myeloma can be quite challenging when it presents together with other comorbid diseases like kidney failure. This is especially due to MM's age of onset targeting the older part of the population(5)(6), as by this age an individual is prone to have multiple diseases;
due to this, MM can be found at a much more advanced stage that can be detrimental and can cause an increase in mortality rate. Furthermore, the asymptomatic nature of presentation(6) in certain patients and the similarity of presenting symptoms with other comorbidities can cause the differential diagnosis and treatment of illnesses in these groups of patients difficult.
This case report highlights the diagnostic challenges and complexities in managing a 66-year-old female patient with multiple comorbidities including Chronic Kidney Disease (CKD) stage 2, Type 2 Diabetes Mellitus, Arterial hypertension and Chronic Coronary Heart Disease, complicated by nephropathy, anaemia, and elevated Erythrocyte Sedimentation Rate (ESR). The patient was presenting with severe proteinuria despite having a good control of her blood sugar levels, which lead to the physicians to consider an alternative diagnosis. A sternal puncture was performed, and she was ultimately diagnosed with Multiple Myeloma.
This study is unique due to the atypical presentation of MM in a patient with well-controlled diabetes mellitus and CKD, emphasizing the diagnostic dilemmas met in distinguishing MM-related kidney damage from diabetic nephropathy. Such cases showcasing the coexistence of MM and preexisting CKD are rare, underscoring the need for thorough investigation of symptoms in patients with overlapping chronic conditions.
Written informed consent was obtained from the patient, and the CARE guidelines have been followed in writing this article.
II. THE CASE
A 66-year-old woman with CKD stage 2 was admitted to the nephrological unit with complaints of lower extremity oedema constant for about one and a half months, fatigue, exertional dyspnoea and significant fluctuations in her laboratory markers. These fluctuations started one year ago and were treated on an outpatient basis. The patient has a history of Type 2 Diabetes Mellitus, Arterial Hypertension, Chronic Coronary Heart Disease (complicated by
Heart Failure: Functional class II), atherosclerotic cardiosclerosis, frequent ventricular extrasystole, aortic and mitral regurgitation. The patient has no relevant psychosocial or family history for oncological diseases.
Her day-to-day medications include anti-diabetic therapy (Metformin, Gliclazide), Aspicard 75 mg for antiplatelet purposes, Rosuvastatin 10 mg, Trimetazidine 35 mg morning and evening, Spironolactone 25 mg, Torsemide 5 mg in the morning.
After evaluating the patient, she was found to be conscious and alert, with a rhythmic pulse of 75 beats per minute. The respiratory rate was 17 breaths per minute, blood pressure was recorded as 110/90 mmHg. Lung sounds were clear, and heart sounds were muted and rhythmic upon auscultation. No tenderness was detected at the renal angle. Pitting oedema of the shins were noted. The rest of the examination revealed no noteworthy findings.
Laboratory investigations were conducted (Table 1). This revealed changes in general urine analysis such as proteinuria, increased pH and presence of erythrocytes; complete blood count showed signs of mild normocytic hypochromic anaemia and increased ESR; biochemical blood test unveiled decreased total protein.
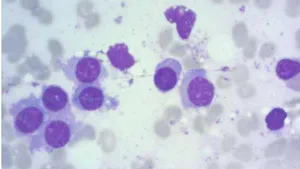
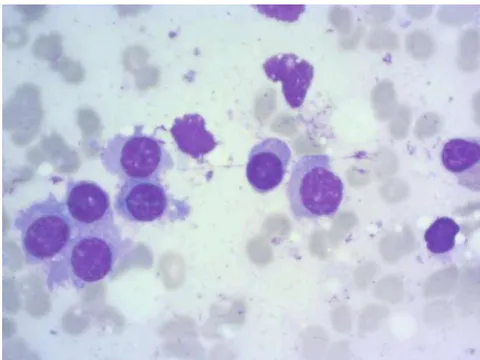
The diagnosis upon admission was chronic tubulointerstitial nephritis due to the preexisting nephropathy of combined genesis (Diabetes mellitus, Arterial Hypertension). The patient's hypertension was effectively managed and within normal limits. She also had good glycaemic control (7%), but the level of proteinuria (2.1 g/l) was not consistent with this range of HbA1c, so alternative diagnoses were considered. After consultation with a haematologist, she was recommended to undergo sternal puncture, which revealed changes consistent with diffuse-focal form of Multiple Myeloma stage 2. (Figure 1) (Table 2)
Laboratory Analysis (Table 1)
| Complete Blood Count | WBC (Leukocytes) | 8.46x10*9/l (4-9) x10*9/l) |
| RBC (Erythrocytes) | 4.01x10*12/l (3.7-4.9) x10*12/l) | |
| HGB (Haemoglobin) | 104g/l ((120-160) g/l) | |
| HCT (Haematocrit) | 34.1% ((32-47)%) | |
| MCV (Mean Cell Volume) | 85 Fl. ((82-92) Fl.) | |
| MCH (Haemoglobin content in RBC) | 25.9 pg ((28-32) pg) | |
| MCHC (Haemoglobin concentration in RBC) | 305g/l ((320-360) g/l) | |
| PLT (platelets) | 439x10*9/l ((150-450) x10*9/l) | |
| RDW-CV | 16.8% ((11.5-14)%) | |
| NEUT (Neutrophils) | 67% (45-70)%) | |
| LYPMH (Lymphocytes) | 19% ((18-40)%) | |
| MONO (Monocytes) | 9% ((3-8)%) | |
| ESR | 58 (2-15) | |
| General Urine Analysis | pH | 8 (5.5-7) |
| Protein | 2.1g/l (0-0.15g/l) | |
| Glucose | 0 mmol/l (0-1.4mmol/l) | |
| Blood | 10 RBC/μl (0-5 RBC/μl) | |
| Colour | Yellow | |
| Transparency | Cloudy | |
| HbA1C | Glycated haemoglobin | 7% |
| Biochemical Blood Test | Total protein | 58g/l ((65-85) g/l) |
| Albumin | 34g/l ((35-53) g/l) | |
| Urea | 7.4mmol/l (1.7-8.3) mmol/l) | |
| Creatinine | 78μmol/l ((53-97) μmol/l) | |
| Cholesterol | 4.1mmol/l ((3.12-5.2) mmol/l) | |
| Triglycerides | 1.93mmol/l ((<=1.52mmol/l) | |
| C-reactive protein | 2.3mg/l ((0-6) mg/l) | |
| Blood glucose | 6.7mmol/l ((3.5-6.2) mmol/l) | |
| Alkaline phosphatase | 146 U/l ((30-120) U/l) | |
| Iron | 13.4μmol/l ((9-30.4) μmol/l) | |
| Ferritin | 55.2ng/ml ((10-120) ng/ml) |
| Cells | Values |
| Blast cells | 0.2% (0.1-1.1%) |
| Neutrophils: Myelocytes | 9.20% (7-12.2%) |
| Neutrophils: Metamyelocytes | 1.80% (8-15%) |
| Neutrophils: Band | 7.60% (12.8-23.7%) |
| Neutrophils: Segmented | 8.20% (13.1-24.1%) |
| Eosinophils | 1.40% (0.5-5.8%) |
| Basophils | 0% (0-0.5%) |
| Monocytes | 1.40% (0.7-3.1%) |
| Lymphocytes | 19.40% (4.3-13.7%) |
| Plasma cells | 25.2% (0.1-1.8%) |
| Normoblasts: Basophilic | 4.0% (1.4-4.6%) |
| Normoblasts: Polychromatophilic | 21.6 (8.9-16.9%) |
| Total erythropoietic cells | 25.6% (14.5-26.5%) |
| Functional activity of megakaryocytes | 12.82% |
| Weakly functioning megakaryocytes | 17.95% |
| Leuko-erythroblastic ratio | 2.91 (2-4.5) |
| Neutrophil maturation index | 0.7 (0.5-0.9) |
| Erythrocyte maturation index | 0.84 (0.7-0.9) |
The patient was recommended to undergo treatment with Bortezomib 1.75mg intravenously jet and Cyclophosphamide 200mg intravenously drip on , , and days; Dexamethasone 20mg intravenously drip on days and days, which is the standard treatment regimen(7) for MM. Bortezomib is a proteasome inhibitor, which has been proved to be beneficial in patients with MM, complicated by renal insufficiency(8). Cyclophosphamide is given for its antineoplastic effect and Dexamethasone for its anti-inflammatory effect. Additionally, Furosemide 40mg intravenously to manage fluid overload and Omeprazole 20mg 1 tablet a day for gastrointestinal protection from prolonged steroid use were also added to treatment regimen.
III. DISCUSSION
Multiple myeloma and CKD are two diagnoses that have overlapping symptoms. In a patient presenting with pre-existing CKD, diagnosing MM can be quite challenging due to similar overlapping symptoms such as proteinuria and oedema. MM in such cases may go completely undiagnosed because of these common presenting features.
Diagnosing multiple myeloma in this 66-year-old patient was particularly challenging due to her complicated medical history disclosing the existence of multiple comorbidities such as heart failure, diabetes, hypertension and the pre-existing CKD. The revealing of multiple myeloma became even less likely due to the absence of classic symptoms.
When the patient 1 arrived at the clinic, her symptoms were attributed to the preexisting CKD and nephropathy secondary to diabetes and hypertension. However, the proteinuria did not align to what would be considered normal in a patient with well-controlled blood glucose levels or with stable blood pressure parameters, raising suspicion for an alternative diagnosis. This case demonstrates how renal manifestations of MM can coexist with diabetic nephropathy, especially with preexisting CKD. The normal glycaemic profile served to highlight the importance of further investigation and re-evaluation of presumed diagnosis when clinical features deviate from expectations.
Furthermore, mild anaemia presenting in this patient projected many red flags that prompted the need for a haematological investigation. Firstly, the anaemia is disproportionate to the stage of CKD; for a patient such as this who is in stage 2 of CKD, a normocytic hypochromic anaemia would be atypical(9) as this often presents at much later stages of CKD due to erythropoietin deficiency.
Additionally, elevated ESR is seen in approximately 85 percent of patients with MM(10) and as well as the aforementioned proteinuria point to a systemic process beyond diabetic nephropathy or heart failure. Although this patient did not have hypercalcemia or bone abnormalities as a presenting feature which is a common initial presentation(11), the triad of anaemia, renal involvement and increased ESR justified the need to rule out haematological malignancies, hence a bone marrow biopsy was undertaken.
Even though there is a significant overlap in symptoms, there is a lack of research done on the topic of Multiple Myeloma and preexisting CKD in the same patient. The majority of existing studies mostly focus on MM-induced kidney damage as kidney disease can occur in upto 50% of patients with MM(12) and these studies don't address the fact that several symptoms are shared between the two diseases that could lead to a misdiagnosis. Further studies should be done examining the relationship between these two conditions. Recent guidelines (KDIGO, IMWG) encourage medical professionals to consider the possibility of MM in patients presenting with Acute Kidney Injury of unknown origin. It's important to note that a lack of awareness among physicians about the possibility of MM in a CKD patient could potentially have a fatal outcome.
IV. CONCLUSION
Overall, this case report emphasizes the difficulties in diagnosing MM in patients that present a history of multiple comorbidities which have similar symptoms, especially in patients suffering from CKD. When a patient presents with unexplained anaemia, increased ESR and proteinuria, it's always important to consider a possible MM diagnosis, especially if the patient is over the age of 60. The rapid diagnosis of such patients allows healthcare providers to offer better treatment modalities leading to lower rates in mortality and better outcomes for the patient as depicted in this case report. This report also serves to demonstrate the importance of thoroughly investigating patients with multiple comorbidities and complex medical histories.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research

Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.

