



IntelliPaper
Abstract
Background/Objectives: Wound treatment has undergone significant advances with the development of dressings and therapies that provide not only simple protective coverage but also actively promote tissue regeneration. This work addresses the classification of dressings, ranging from primary and secondary types to cutting-edge technologies, including bioactive, innovative, 3D-printed, and nanotechnological dressings.
Methods: A structured narrative literature review was conducted by searching major health, nursing, and wound care databases major health, nursing, and wound care databases, complemented by specialized sources.
Results: The review indicates that auxiliary therapies, such as stem cells, growth factors, and cold plasma, are predominantly explored as adjunctive approaches alongside advanced wound dressings, with the literature reporting potential benefits in accelerating healing, especially in complex and chronic wound settings. It also highlights the primary challenges to implementing these approaches, including high production costs, a shortage of trained professionals, limited robust, long-term clinical studies, and regulatory hurdles. Additionally, the environmental impacts of dressing production and disposal were addressed, highlighting the role of biopolymers and nanotechnology as sustainable and ef icient alternatives to traditional methods.
Conclusions: Despite current limitations, future prospects remain promising, with an emphasis on personalized medicine, intelligent monitoring systems, and bioengineering, underscoring the need for more in-depth research and clinical validation to consolidate these innovations in wound care practice.
Explore Digital Article Text
Introduction
Skin wounds, whether acute or chronic, pose a significant global public health problem and are characterized by high morbidity rates, prolonged recovery times, and substantial costs to healthcare systems (Queen et al., 2004; Dhivya et al., 2015; Singh et al., 2017; Sen, 2019). Conditions such as diabetes, venous insufficiency, pressure injuries, and burns further aggravate the scenario, requiring effective, safe, and accessible therapeutic approaches (Bao et al., 2009; Lima et al., 2017; Sierra-Sánchez et al., 2021; Liu et al., 2024; Zhao et al., 2024). In this context, the appropriate choice of dressing is a central element in clinical management, as it not only protects the wound bed against external agents, but also directly influences the cellular processes involved in healing (Queen et al., 2004; Franco; Gonçalves, 2008; Anisuzzaman et al., 2022; Sinha et al., 2022; Herman et al., 2023).
In recent decades, scientific and technological advances have promoted a revolution in wound treatment, with the development of high-tech dressings capable of actively interacting with the wound microenvironment (Ovington, 2007; Jiang; Loo, 2021; Zhang et al., 2021; Tran et al., 2023; Alberts et al., 2025). Innovative, bioactive, 3D-printed dressings composed of nanomaterials or biopolymers have expanded therapeutic possibilities, whether through mechanisms such as the controlled release of drugs, electrical stimulation, incorporation of stem cells, growth factors, or other bioactive agents (He et al., 2023; Yayehrad et al., 2023; Zhang et al., 2023; Astaneh; Fereydouni, 2024; Khushnood, 2024; Alberts et al., 2025). However, despite the promising evidence reported, mainly through in vitro tests, these products still face significant barriers to their large-scale adoption, such as regulatory limitations, scarcity of quality clinical studies, high costs, and lack of professional training (Laurano et al., 2022; Luo et al., 2023; Ruan et al., 2023; Yang et al., 2023; Namgoong et al., 2023; Liu et al., 2024).
Given this scenario, a comprehensive analysis of the main categories of dressings, their classifications, characteristics, incorporated technologies, current limitations, and future perspectives becomes essential. Thus, the objective of this study was to discuss investigations into wound treatment using conventional and technological dressings.
Methodology
This literature review was conducted using a structured narrative approach. Searches were conducted in databases focused on health, nursing, and wound care research. Access was achieved through university libraries, hospital libraries, or institutional portals. In addition to peer-reviewed scholarly articles, reports from relevant medical organizations and government agencies were consulted to address regulatory and clinical guidelines. The search focused on keywords such as "wound dressings," "bio-material," "nanotechnology," and "3D printing," combined with related terms to encompass the history, classification, and future prospects of wound treatment. The inclusion and exclusion criteria were applied to select the most relevant and up-to-date sources in the field.
History
Humanity comprises beings susceptible to various types of injury. Wound treatment is one of the oldest areas in medicine, with evidence of the application of dressings dating back to the earliest stages of human civilization (Majno, 1976). Several studies cite a Sumerian clay tablet dated to 2200 BC as one of the oldest manuscripts on wound treatment, describing a sequence of steps for wound care: washing, dressing, and bandaging (Shah, 2011; Teall, 2014; Ahmad et al., 2020). Ancient Egyptian history contains extensive medical knowledge. This includes the use of various methods and herbs for wound healing (De Paula, 1962; Pertile, 2020). The Edwin Smith Papyrus, also known as the Surgical Papyrus, dates back to approximately 1700 BC and contains a detailed description of 48 cases of injuries, including wounds to the head, throat, collarbone, arm, and chest, along with their corresponding treatments (Feldman & Goodrich, 1999). These same ancient people described using honey, fat, and linen to cover wounds, due to honey’s antibacterial properties and linen’s absorbent capacity (Leake, 1952; Ahmad et al., 2020; Gebarowski et al., 2020). These practices remain in use today and serve as a basis for studies on the efficacy of these materials in topical wound care. Flax fibers, for example, continue to be investigated for application in difficult-to-heal wounds (Gebarowski et al., 2020).
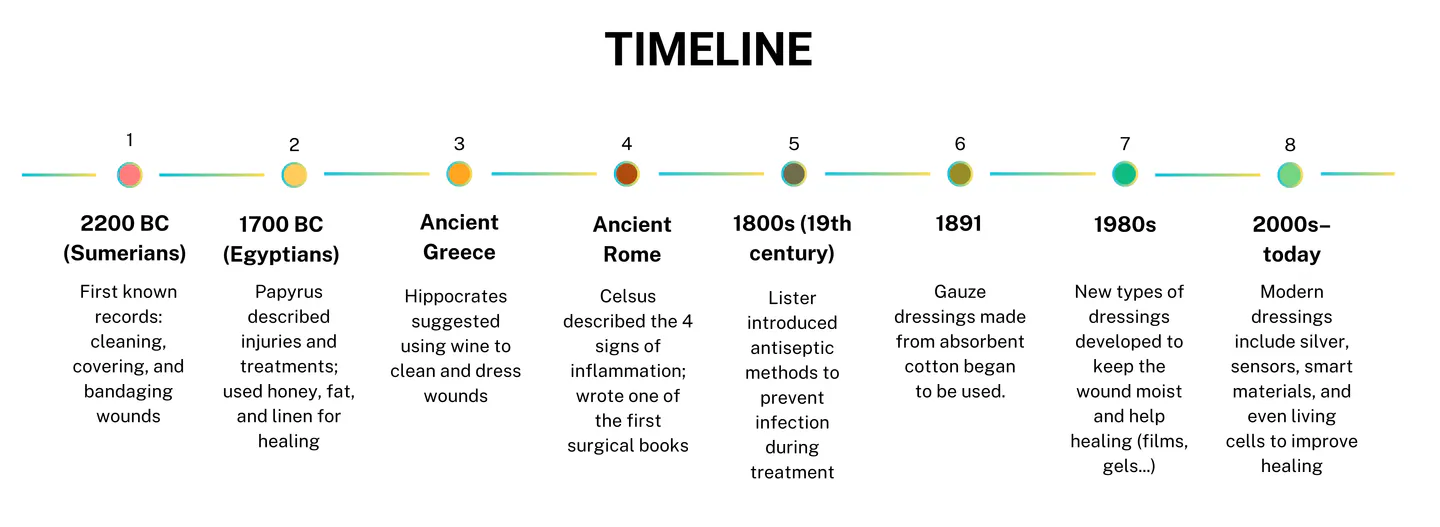
Timeline Highlights Showing the Evolution of Wound Treatment and Dressing Technologies
In Ancient Greece, Hippocrates suggested, in 460-370 BC, the use of wine in the treatment of wounds, both to clean them and to enrich the wool used as a dressing, by boiling, since wine help reduce infection and enhance healing (Majno, 1976; Dhivya et al., 2015). Following the path of ancient civilizations, the Romans also played a prominent role. Cornelius Celsus, a Roman who lived between 25 BC and 50 AD, wrote “De Medicina”, the most significant medical document since the writings of Hippocrates, which was rediscovered by Pope Nicholas in 1443 and printed in 1478 AD, as the first medical and surgical book in history (Kockerling et al., 2013). Celsus is credited with documenting the four cardinal signs of inflammation: rubor (redness), tumor (swelling), calor (heat), and dolor (pain) (Tracy, 2006; Charles et al., 2011). These signs are still used today, reinforcing the importance of these writings.
In the 19th century, a significant advance in wound treatment occurred when Joseph Lister, a professor of surgery in London, introduced the concept of antisepsis in surgical procedures to prevent infections. Using carbolic acid (phenol), Lister sterilized wounds and surgical instruments to prevent sepsis. Additionally, the professor implemented changes to the environment surrounding patients, aiming to make it as sterile as possible (Bhattacharya, 2012). This practice revolutionized wound treatment and laid the foundations for modern surgery. In mid-1891, absorbent cotton-based gauze began to be used to cover wounds (Dhivya et al., 2015). The 20th century witnessed significant advances in the understanding and development of dressings. In the 1980s, the knowledge of the importance of a moist environment for healing led to the development of occlusive and semipermeable dressings, such as film dressings, hydrocolloids, and hydrogels (Queen et al., 2004; Dhivya et al., 2015). It is important to emphasize the importance of maintaining a moist environment for optimal wound healing, a finding reported to date (Lagoa et al., 2024).
Technological innovations mark the century. Research into wound dressings focuses on developing advanced technologies. Examples of these are silver-impregnated dressings for antimicrobial action (Percival et al., 2011; Krishnan et al., 2020); innovative dressings that integrate temperature and pH sensors, in addition to a controlled drug release system, enabling continuous monitoring and personalized treatment of chronic wounds (Mostafalu et al., 2018); dressings with fluorescent nanosensors that glow under UV light when they detect infection, allowing monitoring without the need to remove the dressing (Truskewycz et al., 2021); the use of nanodiamonds embedded in silk fibroin membranes to create dressings that detect infections and promote wound healing (Khalid et al., 2020); in addition to techniques involving the use of tissue engineering technologies using, for example, cells and biomaterials (Hu et al., 2014; Dehkordi et al., 2019; Sindhi et al., 2025). These innovations aim to improve clinical outcomes and patients’ quality of life. These topics will be discussed in more detail in a later session.
Classification of Wounds
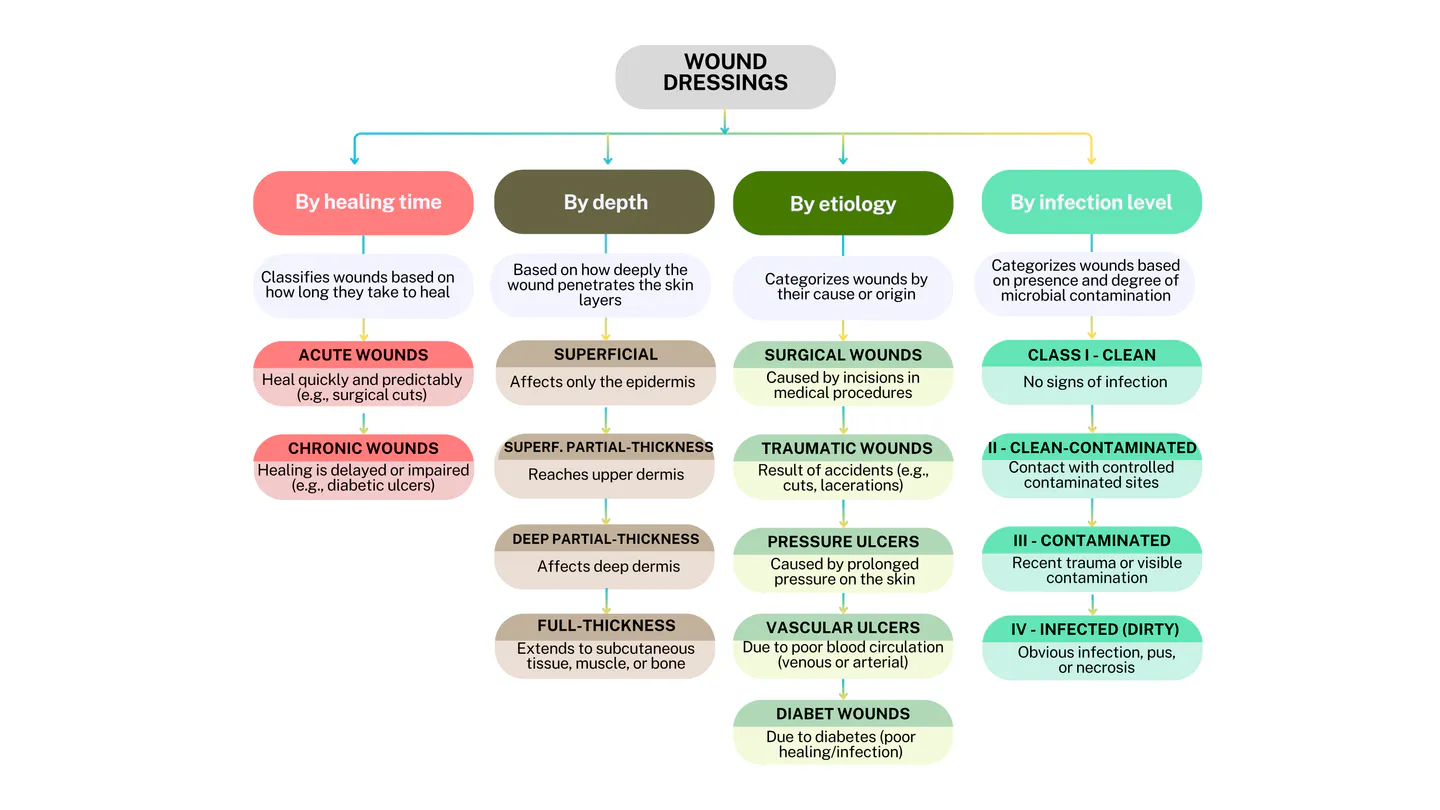
A wound is defined as any discontinuity in the anatomical and functional integrity of the epithelial lining of the skin or mucous membranes, caused by physical, chemical, or thermal damage (Dhivya et al., 2015). Understanding and classifying these wounds has been crucial in the history of medicine, guiding therapeutic interventions and enhancing healing outcomes. Since ancient reports, such as in Egypt, Greece, and Rome, the need to differentiate clean wounds from infected wounds has been observed, as well as the time required for their recovery (Sipos et al., 2004; Tracy, 2006; Charles et al., 2011; Shah, 2011; Kockerling et al., 2013; Hartmann, 2016). With advances in microbiology, physiology, and modern clinical practices, it has become possible to classify wounds based on criteria such as healing time, depth, etiology, and presence of infection, contributing to more specific and practical therapeutic approaches (Lazarus et al., 1994; Cutting; White, 2004; Herman et al., 2023; Figure 2).
Regarding healing time, wounds are classified into two large groups: acute and chronic (Nagle et al., 2023). Acute wounds follow a well-defined healing process, occurring in an orderly and predictable manner, such as surgical wounds, superficial cuts, or lacerations (Justiniano, 2010). Chronic wounds are characterized by impaired tissue-healing capacity, which is generally due to etiologies such as diabetes, persistent pressure, venous reflux, sickle cell anemia, and arterial insufficiency, among others (Bao et al., 2009). Chronic wounds do not heal within the expected timeframe due to factors such as persistent infection, poor tissue perfusion, necrosis, chronic inflammation, microbial infection, and therefore, remain for weeks or months, requiring more complex clinical management (Justiniano, 2010). In this initial stage of wound characterization, it becomes apparent that the type of treatment and dressing applied during the healing process is crucial for a successful recovery, as each type of wound has its unique characteristics.
Given the importance of knowing which type of wound will be treated, more advanced studies are investigating technologies to help better classify these wounds, for example, through a multimodal classifier based on a deep neural network using images of wounds and their corresponding locations, presenting an accuracy that varied between 82.48 and 100% (Anisuzzaman et al., 2022). Regarding depth, some wounds, such as those caused by burns, are classified as superficial, involving only damage to the epidermis; superficial partial-thickness and deep partial-thickness, which affect the dermis; and full-thickness, reaching underlying tissues such as muscles and bones (Merten et al., 1997; Parvez et al., 2024; Rice et al., 2025). Assessing wound depth is crucial for determining injury severity and planning the most appropriate treatment. The classification of wounds by etiology refers to the cause of the wound. These causes can be diverse, including surgical, traumatic, pressure, vascular, and diabetic wounds (Leaper, 2006; Akagi et al., 2012; Boyko et al., 2018; Tobiano et al., 2022; Zaidi & Sharma, 2024).
Schematic Representation of the Main Clinical Criteria used to Classify Wounds, Considering Healing Time, Depth, Etiology, and Infection Level
Surgical wounds are those caused by incisions made during surgeries (Leaper, 2006; Akagi et al., 2012; Tobiano et al., 2022); traumatic wounds are caused by accidental injuries such as cuts or lacerations (Leaper, 2006); pressure wounds, also known as pressure ulcers or bedsores, are lesions on the skin resulting from prolonged pressure on the skin (Boyko et al., 2018; Zaidi; Sharma, 2024); vascular ulcers include venous and arterial ulcers, which are chronic wounds caused by prolonged venous insufficiency, due to poor circulation in the veins, which causes tissue wear (Raffetto, 2010; Robles-Tenorio; Ocampo-Candiani, 2022) and; Diabetic wounds, as the name suggests, are those that occur in patients with diabetes, and are characterized by persistent infection and inflammation, resulting in impaired skin healing (Chaffee et al., 2018).
Regarding the classification of infectious microorganisms, the National Academy of Sciences and the National Research Council of the United States developed the Surgical Wound Classification System (SWC), which was created to represent the bacterial load in a surgical field and was later refined by establishing four classes of wound status: class 1 clean wounds; class 2 clean-contaminated; class 3 contaminated; and class 4 dirty or infected (Herman et al., 2023). The presence of microorganisms in wounds is crucial in the healing process. The quantity and diversity of microorganisms present in any wound depend on the type of wound, its depth and location, and the patient’s immune response (Bowler et al., 2001). The issue is that, if infected by pathogenic microorganisms, wounds have difficulty healing, patient suffering increases, treatment costs become higher, and the treatment process becomes more onerous and expensive, resulting in delayed healing (Bowler et al., 2001; Tom et al., 2019).
An aggravating factor in wound infections is the presence of biofilm-forming microbial species. This is because the biofilm forms a protective layer that protects microorganisms against the action of antimicrobial agents (Justiniano, 2010). The presence of these bacterial biofilms perpetuates the inflammatory state, as the bacteria protected by them are more resistant to antimicrobial treatments (Clinton; Carter, 2015; Jara et al., 2017; Gajula et al., 2020; Thaarup et al., 2022). Given the above, the importance of correctly classifying wounds for choosing the appropriate treatment method, as well as the ideal type of dressing and, consequently, the proper use of topical or oral medications for a successful healing process, becomes clear (Franco; Gonçalves, 2008; Anisuzzaman et al., 2022; Herman et al., 2023).
Wound Treatments
General Principles of Healing
Knowledge about wound healing is constantly evolving, as its basic mechanisms are continually being studied, leading to the development of new therapeutic models (Ho; Hantash, 2013). Wound healing is a complex and dynamic biological process essential for restoring tissue integrity after an injury (Singh et al., 2017). This process occurs in sequential, interdependent phases, each performing specific functions to ensure the effective repair of damaged tissue (Gonzalez et al., 2016; Figure 3). Physiologically, the healing process is divided into four main phases: homeostasis, inflammation, proliferation, and remodeling (Singh et al., 2017). Homeostasis occurs immediately after injury to stop bleeding. Platelets aggregate at the wound site, releasing clotting factors that promote fibrin clot formation, which is crucial for stopping blood loss and providing a temporary matrix for cells involved in the healing process. This phase is critical in preventing infection and preparing the wound bed for subsequent stages of the healing process (Daunton et al., 2012; Singh et al., 2017; Locatelli et al., 2021).
The inflammatory phase begins immediately after homeostasis has been established. The primary function of this stage is to prevent infection by infiltrating the site with neutrophils, aiming to destroy debris and pathogenic bacteria. This destruction process can occur in three ways: by phagocytosis; by the formation of chromatin and protease traps that capture and suppress bacteria; or by the release of toxic substances to them (Ho; Hantash, 2013; Singh et al., 2017). In general terms, the function of neutrophils in the inflammation phase is to promote the “cleaning” of wounds. Inflammation of a wound is a typical example of a biological process of stimulus-response. For example, when microorganisms infect wounds, the immune system reacts by trying to eliminate these invaders (Tracy, 2006). Still in the inflammation phase, known as late inflammation, vasodilation occurs, increasing blood flow and recruiting immune cells, such as macrophages, which improve healing conditions (Daunton et al., 2012).

Simplified Flowchart Showing the Main Stages of Skin Wound Healing, from Injury to Complete Tissue Regeneration (Based on Singh et al. 2017, Campos et al. 2007, and others)
The proliferative phase is accentuated around the fourth day after injury and is divided into four stages: reepithelialization, angiogenesis, granulation tissue formation, and collagen deposition (Campos et al., 2007). The proliferative phase is the primary phase of reepithelialization, during which the wound surface is covered, vascular function is restored, and granulation tissue forms (Landén et al., 2016). Reepithelialization consists of the proliferation of cells (keratinocytes) that migrate from the edges of the wound to cover it; angiogenesis is the process by which endothelial cells form new blood vessels, which are essential for the circulation of blood, oxygen, and nutrients in the affected area (Landén et al., 2016). Around the fourth day after the injury, granulation tissue begins to form, driven by fibroblast proliferation (Gonzalez et al., 2016). The collagen deposition of this phase refers to the initial production of a thinner and less resistant type of collagen, specifically type III collagen, which aims to achieve the skin’s initial firmness (Campos et al., 2007; Daunton et al., 2012).
Finally, the last phase of the healing process, remodeling, involves the gradual replacement of the initial collagen (type III) with thicker and stronger collagen types I and II, thereby increasing the wound’s tensile strength (Campos et al., 2007). Collagen plays a fundamental role in the healing process, and its deficiency or dysregulation hinders healing, complicating the process (Mathew-Steiner et al., 2021). As a result, adjuvant collagen-based therapies have been employed to regulate processes during healing and, consequently, promote more efficient healing (Mathew-Steiner et al., 2021; Gajbhiye & Wairkar, 2022).
Another critical point in the healing process is that, historically, it was believed that the wound healing process would be more efficient when the lesion remained dry and formed a crust, considering that this would prevent infections and accelerate tissue closure, as reported in an Egyptian medical text called the Edwin Smith Surgical Papyrus in 1615 BC (Dhivya et al., 2015). However, in recent decades, scientific evidence has shown that this concept is incorrect and that, in reality, maintaining a moist environment in the wound promotes faster, more efficient healing with less scar formation (Winter, 1962; Boateng et al., 2008; Junker et al., 2013; Dhivya et al., 2015; Frykberg and Banks, 2015; Nuutila and Eriksson, 2021). The study considered pioneering in this new approach of a moist environment rather than a dry one is that of Winter (1962), who demonstrated that wounds kept in a humid environment epithelialized faster than those kept in a dry environment. Later studies have shown that warm, moist environments in wounds facilitate quicker and more effective healing (Boateng et al., 2008; Nuutila and Eriksson, 2021).
In summary, wound healing is a highly coordinated process that depends on the interaction of several cell types and chemical mediators. Understanding the general principles of this process is essential for the implementation of effective therapeutic strategies and for the promotion of adequate healing (Winter, 1962; Daunton et al., 2012; Ho; Hantash, 2013; Gonzalez et al., 2016; Singh et al., 2017; Locatelli et al., 2021; Mathew-Steiner et al., 2021; Nuutila and Eriksson, 2021).
Traditional and Modern Techniques
While conventional methods remain fundamental, modern approaches offer promising alternatives for complex and difficult-to-heal wounds (Panasci, 2014; Bigliardi et al., 2017; Thomas et al., 2021; Mayer et al., 2024). Traditional wound care techniques include adequate cleansing, debridement, and the use of basic and simple dressings, such as sterile gauze, to protect the wound, absorb exudates, and promote healing (Wilkins; Unverdorben, 2013; Wolcott; Fletcher, 2014; Dhivya et al., 2015). When the wound is covered with a dressing, it is continuously exposed to proteinases, chemoattractants, and growth factors, which are lost when the wound is exposed to the air (Dhivya et al., 2015). Therefore, the appropriate use of dressing aids supports the healing process. The treatment process still follows the same pattern; however, with increasingly advanced technologies, the aim is to achieve greater cure success and increased patient comfort.
Wound cleaning is a fundamental part of the traditional wound bed preparation process, removing dirt and bacteria that are lightly adhered to the wound, thereby preventing microbial infections (Panasci, 2014; Wolcott & Fletcher, 2014). However, this cleaning is not the decontamination of the wound, but rather the removal of the superficial layer of cellular residues or bacteria that may have accumulated on the wound bed (Panasci, 2014). Wound cleaning is still part of wound treatment, even in the most current techniques, and can commonly be done using various solutions, such as drinking water, sterile saline solution, iodine-based antiseptics, solutions containing surfactants, etc. (Silva et al., 2014; Panasci, 2014; Bigliardi et al., 2017; Mayer et al., 2024).
Debridement is considered a standard procedure in the treatment of wounds, especially chronic ones, and involves removing dead tissue and senescent bacteria from the wound bed to promote the formation of healthy granulation tissue and optimize wound healing (Wilkins; Unverdorben, 2013; Fumi et al., 2014). This procedure ranges from more conventional, “rustic” practices to more advanced ones. Thomas et al. (2021) report traditional forms of debridement, such as mechanical debridement, which involve more painful and advanced procedures. The conventional mechanical debridement method can cause significant pain for patients, as it involves, for example, the use of wet gauze on the wound bed. As the gauze dries and adheres to the wound’s necrotic tissue, it is removed to remove this dead tissue (Atkin, 2014). Due to the discomfort generated by this procedure, more advanced techniques have been developed. Thomas et al. (2021) report that newer debridement methods, such as enzymatic debridement with collagenase, low-frequency ultrasound, hydrosurgery, and larval debridement, are efficient techniques for preparing the wound bed more quickly and causing less patient pain. However, the authors also demonstrate low consistency among these methods regarding patient safety. Table 1 summarizes traditional and modern wound care techniques.
| Aspect | Traditional Techniques | Modern Techniques |
|---|---|---|
| Wound cleansing | Uses water, saline, or simple antiseptics to remove surface debris | Still applied, but with broader use of targeted and specialized solutions |
| Debridement | Mechanical method (e.g., dry gauze); simple but often painful | Includes enzymatic, larval, surgical, or ultrasound-assisted methods; more effective and less painful |
| Type of dressing | Basic sterile gauze, low-cost and protective | Advanced dressings (e.g., hydrogels, foams, bioactive); multifunctional and technology-based |
| Patient comfort | Lower comfort due to pain during dressing changes and poor conformity | Greater comfort, better anatomical fit, and fewer dressing changes needed |
| Infection control | Limited; mostly depends on cleansing | Actively reduces microbial load and biofilms, supporting healing |
| Healing speed | Slower, especially in chronic wounds | Promotes faster healing by improving the wound environment |
| Cost and accessibility | Low cost and widely available | Higher cost and limited availability, especially in resource-limited settings. |
| Treatment customization | A less personalized, general approach for most wounds | Greater treatment individualization based on wound type and patient condition |
| Limitations | Less effective in complex cases; higher discomfort | Requires trained professionals and may have specific contraindications |
Comparative Summary of Traditional and Modern Wound Care Techniques
Based on Panasci (2014), Wilkins and Unverdorben (2013), Wolcott and Fletcher (2014), Dhivya et al. (2015), Thomas et al. (2021), and Mayer et al. (2024)
In addition, surgical debridement techniques, as well as chemical, osmotic, and oxidative debridement methods, among others, are also being studied (Mayer et al., 2024). It is worth noting that the debridement procedure is essential for reducing bacterial load, including biofilm-forming bacteria, which are necessary for healing, especially in chronic wounds (Eriksson et al., 2022; Mayer et al., 2024). Reducing this load helps reverse a chronic wound environment into an acute condition, allowing the wound to undergo the normal healing process (Thomas et al., 2021). Therefore, research has been advancing to make this procedure as efficient and comfortable as possible. A recent study demonstrates professional consensus on efficient debridement techniques, such as selective sharp and surgical debridement, which provide greater patient comfort. However, the authors also note that, in some instances, such as in patients with coagulation difficulties or those with injuries involving exposed bones, ligaments, or tendons, these procedures may be contraindicated (Mayer et al., 2024).
Regarding the use of dressings as part of treatments, there is a variety of these dressings ranging from the cheapest, most common and traditional ones such as gauze (Queen et al., 2004; Jones, 2006; Atkin, 2014; Parkale et al., 2023) to others that are more technological, enriched with enhancing substances, expensive and with more limited access, such as hydrogels, hydrofibers, bioactive, antimicrobial, tissue engineering dressings, foams and semipermeable films, etc. (Bülbül et al., 2022; Parkale et al., 2023; Zhao; Sun, 2024). This will be discussed in more detail in a later session. It is important to emphasize that the best procedure and dressing for wound treatment and healing should not be based on a single factor of the wound or on a specific function of the adopted method or dressing. The patient’s wound, their reality, and their unique needs must also be considered (Queen et al., 2004).
Auxiliary Therapies in the Treatment of Wounds
In addition to what was mentioned above, wound treatment can also include modern, sophisticated auxiliary therapies to optimize the healing process (Table 2). These therapies include negative pressure therapy (Oliveira, 2010; Lima et al., 2017; Normandin et al., 2021; Wu et al., 2022), oxygen therapy (Smet et al., 2017; Nagarsheth et al., 2024), larval therapy or biodebridement (Bazalinski et al., 2023; Lam et al., 2025), low-level laser therapy (Hopkins et al., 2004; Misra et al., 2023), cold plasma therapy (Haertel et al., 2014; Martínez et al., 2024), growth factor therapies (Goldman, 2004; Park et al., 2017; Yamakawa; Hayashida, 2019) and stem cell therapies and tissue engineering (Riedl et al., 2021; Sierra-Sánchez et al., 2021; Downer et al., 2023; Soriano et al., 2023). These auxiliary therapies, also known as adjuvant therapies, aid in healing various types of wounds (Lima et al., 2017).
| Therapy | Mechanism of Action | Clinical Indications | Practical Considerations |
|---|---|---|---|
| Negative Pressure | Pulls out fluids, improves blood flow, and promotes healing | Complex or draining wounds | Needs proper technique; may cause complications |
| Oxygen Therapy | Delivers oxygen to support cell repair and tissue growth | Surgical wounds, ischemic tissues | Effects vary; primarily used in specific cases |
| Larval Therapy | Larvae clean dead tissue and reduce bacteria | Chronic wounds with necrosis | May cause discomfort for some patients |
| Low-Level Laser | Stimulates cells, boosts collagen, and reduces inflammation | Slow-healing or chronic wounds | Requires equipment and trained staff |
| Cold Plasma | Destroys microbes and biofilm, helps tissue regeneration | Infected or chronic wounds | Still experimental in many settings |
| Growth Factors | Triggers healing signals to speed up recovery | Hard-to-heal wounds | Costly and still under study |
| Stem Cells & Bioengineering | Rebuilds tissue and modulates inflammation | Severe or non-healing injuries | Complex and expensive; not widely available |
Summary of Auxiliary Therapies Applied in Wound Management, Including Mechanisms of Action, Clinical Indications, and Practical Considerations
Based on Oliveira (2010), Panasci (2014), Lima et al. (2017), Bazalinski et al. (2023), Mayer et al. (2024), and others
Negative pressure therapy (NPT) is a technique used since the 1990s that promotes healing by applying uniform negative pressure to the wound (Normandin et al., 2021; Wu et al., 2022). It is a non-invasive method that applies negative pressure to the wound to remove excess fluid in difficult-to-heal wounds (Astasio-Picado et al., 2022). The main indications for NPT are complex wounds, including pressure ulcers, diabetic wounds, open abdomen, traumatic wounds, skin grafts, burns, surgical wound dehiscence, and necrotizing wounds (Lima et al., 2017). This is because this technique, for example, promotes arterial vasodilation in the affected tissues, thereby boosting blood circulation in the area and improving oxygenation (Oliveira et al., 2010). In addition to these benefits, NPT reduces edema and exudate, reduces bacterial clearance, stimulates granulation tissue formation, and reduces inflammation (Lima et al., 2017; Wu et al., 2022). In general, NPT is considered a safe therapy; however, some reports demonstrate complications after its use. The work by Normandin et al. (2021) highlights some of these reports, including toxic shock syndrome, enteric fistula, and hemodynamic instability. However, these authors clarify that these complications were associated with poor patient selection or an inadequate technique for the case.
Oxygen therapy is another adjunctive technique in wound treatment. It presents promising results from both hyperbaric oxygen therapy (oxygen administered through the patient’s inhalation) and topical application (Smet et al., 2017; Gupta et al., 2022; Nagarsheth et al., 2024). This is because oxygen is essential for wound healing, as this element is involved in several biological processes, such as protein synthesis, cell multiplication, angiogenesis, reduction of tissue degradation enzymes, reduction of inflammation, promotion of collagen synthesis and, consequently, in aiding the formation of granulation tissue and wound closure (Castilla et al., 2012; Gupta et al., 2022). However, it is essential to note that the relationship between oxygen therapy and wound healing remains complex and warrants further attention regarding its actual effect on the various phases of the healing process. Most studies are limited to surgical wounds, making it challenging to generalize the findings to other types of wounds or in vitro or animal tests (Yip, 2015).
Larval therapy is a procedure that uses disinfected fly larvae, particularly those of Lucilia sericata, to remove necrotic tissue from the wound bed (Nezakati et al., 2020; Gazi et al., 2021; Jafari et al., 2022; Bazalinski et al., 2023). The larvae of these flies are introduced into the wound, where they feed, removing dead tissue and helping to reduce bacterial infection (Nigam, 2021; Bazalinski et al., 2023). As mentioned in the previous topic, debridement is often essential in chronic wounds, and this treatment step can cause significant pain for the patient. Larval therapy, also known as biodebridement, presents an alternative to conventional debridement, aiming to remove dead tissue efficiently while minimizing patient pain (Lam et al., 2025). Studies have shown promising results for this debridement technique; however, there is still considerable resistance to its application due to the psychological discomfort it causes for patients and health professionals (Nigam, 2021; Bazalinski et al., 2023).
Low-level laser therapy (LLLT), also known as photobiomodulation, is a therapeutic approach that uses low-power light, typically in the 600–1000 nm range, to promote wound healing by stimulating tissue growth (Chung et al., 2012). Its mechanism of action involves the absorption of light by opsins, generating cellular chromophores, mainly cytochrome c oxidase in mitochondria, which results in increased ATP production, mild reaction with reactive oxygen species (ROS), and increased nitric oxide (Hamblin, 2017). In addition, LLLT promotes wound healing by stimulating fibroblast proliferation, increasing collagen synthesis, enhancing vascularization in affected areas, facilitating contraction of surrounding tissues, and reducing inflammation (Hopkins et al., 2004; Yang et al., 2022; Misra et al., 2023). A study found that after LLLT, the average healing time for complex skin wounds was 48 days (Otsuka et al., 2022).
Cold plasma therapy, also known as non-thermal atmospheric plasma, is a technique that uses a partially ionized gas at room temperature to treat living tissue (Haertel et al., 2014). Among its benefits, it reduces bacterial load and destabilizes biofilms, thereby promoting wound sterilization (Spiegel et al., 2025). Additionally, it functions as an antiseptic, stimulates the proliferation and migration of skin cells, activates integrin receptors, and promotes angiogenesis (Haertel et al., 2014). In addition to treating exposed wounds, cold plasma treatment exhibits selective cytotoxicity in cancer cells, for example, by inducing the production of reactive oxygen and nitrogen species, which results in oxidative stress within these cells (Martínez et al., 2024).
Factor therapy is an approach that utilizes signaling molecules to stimulate cellular processes essential for wound healing (Goldman, 2004; Yamakawa & Hayashida, 2019). For example, they function as potential supplements to standard treatments for chronic wound healing (Mullin et al., 2024). Growth factors act as triggers that initiate biochemical reactions throughout the phases of healing (Vaidyanathan, 2021). Depending on their structure, they can be administered in various ways, such as particle systems, scaffolds, hydrogels, and different strategies (Park et al., 2017). Some of these growth factors are PDGF (platelet-derived growth factors), VEGF (vascular endothelial growth factor), EGF (epidermal growth factor) and FGF (fibroblast growth factor), which act on cells such as platelets, macrophages, keratinocytes and fibroblasts, resulting in the activation of macrophages to release growth factors, in the promotion of fibroblast proliferation and the production of extracellular matrix, in the promotion of re-epithelialization, in the proliferation of keratinocytes and vascular endothelial cells, among others (Park et al., 2017).
Stem cell therapy and tissue engineering are innovative approaches to restructuring skin integrity in difficult-to-heal wounds. Stem cells, specifically mesenchymal stem cells (MSCs), derived from tissues such as bone marrow and adipose tissue, are notable for their role in wound healing due to their ability to differentiate into various cell types and secrete bioactive factors that promote tissue regeneration (Marti et al., 2011; Maxson et al., 2012). The excretion of bioactives contributes to immune modulation, tissue remodeling, and cellular homeostasis during the regeneration of affected tissues (Han et al., 2022). The combination of differentiation capacity and the secretion of bioactive factors enables MSCs to be utilized in therapies for regenerating soft tissues, including skin, muscles, and blood vessels (Riedl et al., 2021; Rehman et al., 2023).
Tissue engineering involves combining biomaterials, cells, and growth factors to create mechanisms and structures that can replace or regenerate tissues damaged by various conditions, ranging from skin to internal organs (Olson et al., 2011; Borges et al., 2023). It plays a vital role in regenerative medicine, as it is used in various ways, including the development of biocompatible scaffolds that support cell adhesion, proliferation, and differentiation, thereby facilitating the formation of new functional tissue (Krishani et al., 2023). Biomaterials used in tissue engineering can be natural, synthetic, or a combination of both types (Downer et al., 2023). Examples of this therapy include skin substitutes used to treat burns or chronic wounds, such as autologous cultured epithelial substitutes, which consist of keratinocytes and fibroblasts; autologous skin substitutes, composed of biomaterials; and allogeneic cultured dermal substitutes, composed of biomaterials and fibroblasts (Sierra-Sánchez et al., 2021). It is essential to note that these auxiliary therapies can be applied independently as clinical procedures or in conjunction with wound dressings (Garcia et al., 2016; Park et al., 2017; Catanzano et al., 2021).
Classification and Types of Dressings
Choosing the ideal dressing for wound treatment is an ongoing challenge in clinical practice, as this choice represents only one component of a comprehensive therapeutic plan and is associated with various models, benefits, and contraindications (Queen et al., 2004). In addition, there is significant heterogeneity in access, choice, and use of these dressings across regions of the world, driven by factors such as resource availability, local guidelines, cultural practices, and socioeconomic factors (Queen et al., 2004; Koka et al., 2016; Bishop, 2023). It is known that an ideal dressing should perform several functions, mainly to treat wounds efficiently and economically and to be easily removed with minimal inconvenience to the patient (Bülbül et al., 2022). Furthermore, it is expected to promote moisture balance and oxygen exchange, stimulate growth factors, prevent infections, facilitate debridement, promote granulation tissue formation, and promote re-epithelialization (Shi et al., 2020). However, as the healing process is not static, it requires different conditions at each healing phase. Consequently, a single dressing cannot perform all these functions (Gonzalez et al., 2016; Shi et al., 2020; Tottoli et al., 2020).
Furthermore, the diversity of products available on the market and patients’ social conditions make choosing a dressing a complex task (Shi et al., 2020; Sinha et al., 2022). Selecting the wrong dressing can lead to several negative consequences, including prolonged healing time, increased risk of infection, and higher treatment costs (Lima et al., 2017; Nussbaum et al., 2018; Atkin et al., 2019; Santos, 2022; Lagoa et al., 2024). In general, choosing the ideal dressing involves four basic principles: dehydrated wounds require dressings that provide hydration; wounds with high exudate production will require an absorbent dressing; infected wounds will need antibiotic dressings; necrotic wounds or those with visible dirt will require debridement (Morin; Tomaselli, 2007; Sood et al. 2014). Therefore, understanding the phases of the healing process, its classification, and the types of dressings available on the market is crucial for effectively treating various wound types.
General Functions of Dressings
Dressings play a fundamental role in the wound-healing process, acting as physical barriers that protect the wound bed from external agents, such as microorganisms, chemical contaminants, and mechanical trauma (Boateng et al., 2008; Dhivya et al., 2015; Ferraz, 2025). This protection is essential for preventing infections and promoting an environment conducive to tissue regeneration. Furthermore, dressings help maintain local temperature and absorb exudates, contributing to wound homeostasis and facilitating the healing process (Boateng et al., 2008; Dhivya et al., 2015; Ghomi et al., 2019; Tan et al., 2019; Gou et al., 2024; Alberts et al., 2025).
Maintaining a moist wound environment is one of the most essential functions of modern dressings. Studies have shown that adequate moisture accelerates epithelialization and reduces crusting, promoting more efficient healing and greater patient comfort (Winter, 1962; Boateng et al., 2008; Dhivya et al., 2015; Nuutila; Eriksson, 2021). Dressings that maintain this moist environment, such as hydrocolloids and hydrogels, are particularly effective (Tan et al., 2019; Guillen et al., 2022).
In addition to protecting and maintaining moisture, dressings also perform functions such as debridement of necrotic tissues, odor control, and controlled release of therapeutic agents (Dhivya et al., 2015; Jiang; Loo, 2021; Bhoyar et al., 2023; Koumaki et al., 2023; Alberts et al., 2025). For example, dressings impregnated with antimicrobial substances, such as silver, help reduce bacterial load in the wound, preventing infections and promoting faster healing (Jiang; Lo0, 2021; Alberts et al., 2025). Therefore, knowing the types of dressings available and their optimal application becomes essential for successful wound treatment.
Types of Dressings
In general, dressings are classified into several categories based on their class, behavior, clinical performance, physical form, and origin (Boateng et al., 2008; Ghomi et al., 2019; Tan et al., 2019; Table [tab:classification-dressings]). Based on the class, they are divided into primary, secondary, and island dressings (Boateng et al., 2008; Vowden; Vowden, 2017; Shi et al., 2020). Primary dressings are in direct contact with the wound bed (Fahimirada; Ajalloueian, 2019). Therefore, their functions include promoting a suitable environment for healing, controlling moisture, absorbing exudate, releasing bioactive agents, and acting as a barrier against microorganisms (Boateng et al., 2008). Examples of primary dressings include foams, hydrofibers, micronized collagen, hydrogels, hydrocolloids, alginates, nanosilver, and films (Boateng et al., 2008; Frykberg; Banks, 2015; Vowden; Vowden, 2017).
| Classification Criteria | Types | Key Characteristics | Examples |
|---|---|---|---|
| By class | Primary | Contact with the wound bed | Foams, hydrogels, and hydrocolloids |
| Secondary | Fixation, support | Gauze, bandages, adhesive tapes | |
| Island | Primary + secondary | Self-adhesive with central pad | |
| By behavior | Passive | Basic protection | Gauze, tulle |
| Interactive/Bioactive | Healing stimulation, substance release | Nanofibers, hydrogels | |
| By clinical performance | Absorbent | Controls exudate, prevents maceration | Foams, alginates |
| Occlusive | Maintains a moist environment | Hydrocolloids, films | |
| Semi-occlusive | Gas exchange, autolytic debridement | Polyurethane films | |
| Adhesive | Easy fixation, protective barrier | Island dressings | |
| Antimicrobial | Infection control | Silver, iodine, and honey dressings | |
| Physical form and origin | Animal | Protein-based, biocompatible, promotes healing | Collagen |
| Plant | Natural, antimicrobial, good moisture retention | Cellulose | |
| Synthetic | Durable, customizable, controlled drug release | Polyurethane |
Based on Boateng et al. (2008), Ghomi et al. (2019), Tan et al. (2019), Vowden & Vowden (2017), and others.
On the other hand, secondary dressings, such as gauze, cotton, natural and synthetic bandages, adhesive tapes, hydrogel films, and sheet dressings, have as their primary function to provide support, fixation, additional absorption, and protection to the primary dressing (Boateng et al., 2008; Fahimirada; Ajalloueian, 2019; Moradifar et al., 2025). In other words, the primary dressing is designed to be in direct contact with the wound. In contrast, a bandage (secondary dressing), for example, holds the primary dressing in place (Dhivya et al., 2015). It is essential to note that, in some instances, the same product can serve as both a primary and secondary dressing, depending on the clinical situation (Jones, 2014; Shi et al., 2020). Island dressings are those that “unite” primary and secondary dressings in the same dressing, as they have a central absorbent region (island) that is surrounded by an adhesive portion; that is, this type provides treatment of the wound and its fixation (Rippon et al., 2007; Boateng et al., 2008).
Dressings are categorized as passive, interactive, or bioactive based on their behavior. Passive dressings protect the wound without incorporating non-occlusive substances that promote healing, such as gauze and tulle, which are often used to cover wounds (Tan et al., 2019). In contrast, interactive or bioactive dressings, usually occlusive or semi-occlusive, provide or stimulate the release of substances that aid and improve wound healing (Guillen et al., 2022). Based on their clinical performance, dressings can be classified into five categories: absorbent, occlusive, semi-occlusive, adhesive, and antimicrobial (Ghomi et al., 2019). Absorbent dressings are designed to manage excess exudate, maintain a moisture balance in the wound bed, and are essential for healing, as they remove excess fluid, prevent maceration of the peripheral skin, and reduce the risk of infection (Jones, 2014; Gardner, 2016). Examples of these dressings include foam, alginate, and hydrofiber (Frykberg; Banks, 2015). However, they have limitations in dry or low-exudate wounds, as they can adhere to the wound bed and require a secondary dressing for maintenance (Brito et al., 2024).
Occlusive dressings are made of materials that are impermeable to liquids and gases, forming a physical barrier that prevents moisture loss from the wound surface (desiccation) and the entry of microorganisms, providing an ideal microenvironment to promote healing (Helfman et al., 1994; Dhivya et al., 2015; Tan et al., 2019; Guillen et al., 2022). Maintaining occlusion promotes a moist environment that favors epithelialization, as demonstrated by Winter (1962) and in subsequent literature (Boateng et al., 2008; Junker et al., 2013; Dhivya et al., 2015; Frykberg & Banks, 2015; Nuutila & Eriksson, 2021). Occlusive dressings facilitate faster re-epithelialization, promote angiogenesis, aid in collagen synthesis, and decrease the pH of the wound surface, thereby reducing the risk of infection (Dhivya et al., 2015). Examples of these dressings include films, hydrofibers, foams, charcoal, alginates, hydrogels, and hydrocolloids (Tan et al., 2019; Guillen et al., 2022). In the Brazilian health service, hydrocolloids are the most widely used occlusive dressings (Guillen et al., 2022). It is worth noting that these dressings may be contraindicated in highly exudative wounds and may cause skin maceration if used for prolonged periods (Tan et al., 2019; Brito et al., 2024). However, non-occlusive dressings, such as gauze, dry out and adhere to the wound, causing damage during removal and potentially leading to bleeding and pain for the patient (Queen et al., 2004).
In turn, as the name suggests, semi-occlusive dressings, such as polyurethane films, allow a limited degree of oxygen and water vapor exchange between the wound and the environment while remaining impermeable to liquids and bacterial contamination (Colenci et al., 2018; Hodge et al., 2022). In this way, they continue to play a role in moisture retention, providing a moist environment for healing and favoring autolytic debridement and epithelialization of wounds (Bhoyar et al., 2023). These dressings have been increasingly studied and have demonstrated satisfactory results in wound treatment and healing (Madden et al., 1989; Esmaeil et al., 2025). Adhesion dressings, also known as adhesive dressings or island dressings, feature an absorbent central pad and adhesive edges that promote wound stability and protection (Rippon et al., 2007; Matsumura et al., 2014). Although they are easy to apply, as they eliminate the need to cut and prepare surgical tapes to keep the dressing in place, their adverse effects are related to the injuries that they can cause, at the time of their removal, to the epithelium and surrounding healthy skin, generating pain and even increasing the wound area (Waring et al., 2008; Matsumura et al., 2014).
Antimicrobial dressings incorporate active agents that act to reduce the local microbial load, being indicated for infected wounds or those at high risk of infection, and can be presented in the form of films, foams, or hydrogels, among others (Hewish, 2012; Gou et al., 2024; Alberts et al., 2025; Peng et al., 2025). They are varied and composed of different raw materials, including silver, iodine, biguanide, antibiotics, natural products such as medical-grade honey and plant compounds, nanoparticles, chitosan, antimicrobial peptides, and metals, among others (Yousefian et al., 2023; Peng et al., 2025). The importance of this dressing class in treating wounds, especially chronic ones, is well established, and several studies support its use. However, only of antimicrobials are used clinically because most testing is in vitro or, when in vivo, is limited to animal models, and, consequently, there are concerns about their side effects (Gou et al. 2024) among the advances in antimicrobial dressings based on nanotechnology, such as nanoparticles (Alberts et al., 2025).
These are promising avenues for developing innovative dressings that enhance their antimicrobial effect and, consequently, efficient healing (Jiang and Loo, 2021). The use of antimicrobial dressings is essential in the treatment of wounds because infections represent one of the most significant problems in the normal course of the healing process, resulting in increased wound complexity, mortality, length of hospital stay, and treatment costs (Lima et al., 2017; Peng et al., 2025). Regarding other classifications of dressings, based on physical form and origin, they are broadly categorized as gels, ointments, films, foams, and those of animal, vegetable, and synthetic origin (Ghomi et al., 2019). Therefore, based on what has been revealed so far, the correct selection of dressings, taking their classification into account, is crucial for therapeutic success, directly influencing the progression of healing, the prevention of complications, and the reduction of treatment costs.
High-Technology Dressings
High-tech dressings represent a significant evolution in wound care, incorporating scientific and technological advances to optimize healing. These dressings extend beyond their traditional coverage function, offering bioactive properties, real-time monitoring, and controlled drug release, thereby adapting to the specific needs of each injury (Ovington, 2007; Zhang et al., 2021; Tran et al., 2023; Alberts et al., 2025). High-tech dressings are advanced therapeutic devices designed to actively interact with the wound bed, promoting tissue regeneration and preventing complications (Zhang et al., 2021; Tran et al., 2023; Zhang et al., 2025). Among its main types are nanotechnology-based dressings, smart dressings, bioactive dressings, and 3D-printed dressings, among others (Figure [fig:high-tech-dressings]; Jiang; Loo, 2021; Zhang et al., 2021; Chopra et al., 2023; Nie et al., 2023; Alberts et al., 2025).
Among the various advantages that these dressings present, concerning conventional dressings, are the promotion of cell regeneration more efficiently (Colenci et al., 2018; Zhang et al., 2021; Hodge et al., 2022; Zhang et al., 2024; Moradifar et al., 2025); the reduction in the risk of infections provided by dressings with antimicrobial functions (Jiang; Loo, 2021; Gou et al., 2024; Alberts et al., 2025); and; greater patient comfort, due to the reduced need for changes and the greater anatomical adaptation of semipermeable films, for example (Ovington, 2007; Sood et al., 2014; Weller et al., 2020; Lagoa et al., 2024). One of the main disadvantages is the high cost. Advanced dressing technologies are generally expensive, limiting access in some contexts (Laurano et al., 2022; Alberts et al., 2025).
Nanotechnology and Dressings
The definition of nanomaterials is not simple or uniform; however, they are usually defined as structures with at least one dimension in the nanoscale, ranging from 1 to 100 nanometers (Yokel; MacPhail, 2011; Baig et al., 2021). These materials possess specific physical and chemical properties that depend on their size and shape (Baig et al., 2021). For example, some nanoparticle shapes may be more efficient as antimicrobial agents than others. This is observed in the study by Cheon et al. (2019), which demonstrates differences in the antimicrobial activity of silver nanoparticles based on their shape. The results of this study show that spherical nanoparticles exhibit greater action against Escherichia coli strains, followed by disk-shaped and triangular-shaped nanoparticles (Cheon et al., 2019). These authors demonstrated that this difference is due to variations in the release rate of silver ions, resulting from differences in nanoparticle surface area, specifically morphology.
Based on Zhang et al. (2021), Jiang and Loo (2021), Deng et al. (2025), Albert et al. (2025), He et al. (2023), and others

Main types of high-tech wound dressings with key features, applications, and challenges
The research conducted by Barroso et al. (2023) demonstrated that triangular nanoparticles were more effective against strains such as coli. These researchers reported that this greater efficiency may be linked precisely to the triangular shape of the nanoparticles and their sharp edges, which can facilitate interaction with microbial cell membranes. One point worth highlighting when comparing these two studies is that, in the work by Cheon et al. (2019), the spherical nanoparticles were 100 nm in size, and the triangular ones were 200 nm ; that is, the triangular ones are outside what is typically considered a nanomaterial. The triangular nanoparticles of Barroso et al. (2023) were 20 nm in size. Therefore, although some studies indicate that nanoparticles of a particular shape exhibit greater antimicrobial efficacy, others yield different results under specific conditions. Hence, factors such as particle size, ion release rate, target microorganism type, and synthesis method can significantly influence the results (Cheon et al., 2019; Sayed et al., 2022; Barroso et al., 2023). Therefore, investigations into the specific properties of each nanomaterial remain a vast field with significant gaps.
Nanomaterials can be produced in two ways: top-down and bottom-up. In the top-down approach, larger materials are broken down to form nanomaterials using techniques such as mechanical milling and electroexplosion. In contrast, the bottom-up approach produces nanomaterials by constructing nanostructures from smaller individual particles, atoms, or molecules. It can be done using techniques such as chemical vapor deposition (Baig et al., 2021). Various types of nanomaterials are used in technologies collectively referred to as nanotechnologies. Nanotechnology is the science involved in the design, synthesis, characterization, and application of materials whose functional organization, at least in one dimension, is on a nanometric scale (Saini et al., 2010).
Among the properties achieved with nanotechnology, the high surface-to-volume ratio, greater reactivity, ability to penetrate biological tissues and altered optical and mechanical behavior stand out, which makes nanomaterials attractive for diverse applications such as administration, pharmaceuticals, renewable energies, biomedicine, especially in the treatment of wounds, etc. (Sun et al., 2008; Zhang et al., 2023; Khushnood, 2024). Among the technological advances in which nanotechnologies are being increasingly investigated is their application in wound treatment (Leppiniemi et al., 2017; Adamu et al., 2021; He et al., 2023; Astaneh & Fereydouni, 2024; Deng et al., 2025). In this context, they can act as antimicrobial agents (Cheon et al., 2019; Sayed et al., 2022; Barroso et al., 2023; Deng et al., 2025); promoters of cell regeneration or controlled drug release systems (Cheon et al., 2019; Truskewycz et al., 2021; He et al., 2023; Ruan et al., 2023; Deng et al., 2025), and biomolecules directly in the wound bed (Luo et al., 2023).
The application of metallic nanoparticles, such as silver, gold, titanium, cerium, and zinc, for example, has shown efficacy in inhibiting multidrug-resistant microorganisms, while nanofibers and nanostructured hydrogels have been used to provide structural support for tissue regeneration and modulate the inflammatory response (Lu et al., 2022; Liu et al., 2024; Zhang et al., 2024). Investigations into nanofibers are underway, and these materials are emerging technologies with unique characteristics and properties that can be used to develop effective dressings (Zhang et al., 2024). In the study by Partovi et al. (2024), spun nanofibrous dressings demonstrated antimicrobial action against various microbial strains. Additionally, the incorporation of citrate into the nanofibers enhanced the dressing’s porosity, hydrophilicity, and degradability, properties favorable for wound healing. Electrospun nanofibers from gelatin and chitosan-polyvinyl alcohol have also been investigated, yielding satisfactory results with good physical properties and efficient antimicrobial activity against certain microorganisms (Campa-Siqueiros et al., 2020).
Regarding the application of nanoparticles in wound treatment, a summary of the articles discussed in this session is shown in Table [tab:biomaterials-articles]. In the study by Barroso et al. (2023), silver nanoparticles incorporated into bacterial cellulose biopolymers and other components demonstrated satisfactory inhibitory action against . coli and Staphylococcus aureus strains. In this research, the authors attributed this action to several factors, including the triangular shape of the nanoparticles and their sharp edges, which may have facilitated their penetration into the bacterial cell. Nanosilver was also investigated through green synthesis from Ficus benghalensis leaf extract for incorporation into postoperative dressings (Lu et al. 2022). The results demonstrated higher antimicrobial activity and accelerated cell regeneration compared to the isolated plant extract. A study using nanosilver associated with carbon fiber and synthetic drugs achieved bacterial growth inhibition results of 97% for E. coli and 80% for S. aureus (Luo et al., 2022).
Zinc and selenium nanoparticles have demonstrated promising results both in vitro and in vivo for treating pediatric wounds (Ruan et al., 2023). This study showed that nanoparticles formulated in a bioactive chitosan scaffold accelerated wound closure and enhanced collagen deposition when administered in vivo to treat rat wound models. Additionally, it improved re-epithelialization and granulation tissue formation, reduced inflammation and microbial infections in the wound area. Similar results were achieved by Luo et al. (2023), using cerium oxide nanoparticles. The results revealed significant antimicrobial action against S. aureus and E. coli, as well as improved re-epithelialization, cell proliferation, and the formation of new blood vessels. In in vivo tests, the dressing accelerated healing, resulting in 98.5% wound closure after 14 days, whereas the control group showed only 71% closure. Furthermore, the healing hydrogel exhibited rapid gelation, high fluid-absorption capacity, and good mechanical stability.
| Authorship | Country | Type of Study | Objective |
|---|---|---|---|
| (Luo et al., 2023) | China | Biomaterial development and in vitro and in vivo evaluation | To develop and characterize a hydrogel based on polyhydroxyethyl methacrylate (PHEM) and chitosan (CS), incorporated with cerium oxide nanoparticles (CeONPs); to evaluate the antimicrobial properties, biocompatibility, and healing effect of this dressing in chronic wounds |
| Zhao and Sun (2024) | China | Biomaterial development and in vitro evaluation | Demonstrate how combining nanotechnology (AgNPs) with natural biopolymers (chitosan) can offer a more efficient and safe treatment for patients with chronic wounds, especially in nursing care contexts for diabetic patients |
| Liu et al. (2024) | China | Biomaterial development and in vitro evaluation | To develop and characterize a bioactive hydrogel based on chitosan (CS) and hyaluronic acid (HA), incorporated with gold nanoparticles (AuNPs) and fibroblast growth factors (FGFs); to evaluate the effectiveness of the hydrogel in healing diabetic wounds, emphasizing antimicrobial properties and stimulation of tissue regeneration |
| Yang et al. (2023) | China | Biomaterial development and in vitro and in vivo evaluation | To develop chitosan-based wound dressings with titanium nanoparticles (TiO2) for hospital and pediatric use; to evaluate the ability of these dressings to monitor wound temperature, humidity, and pH, in addition to their antimicrobial efficacy, reduce the risk of hospital infections, and improve patient comfort |
| Ruan et al. (2023) | China | Biomaterial development and in vitro and in vivo evaluation | To develop and evaluate chitosan-based antibacterial dressings incorporated with zinc oxide (ZnO) and selenium nanoparticles (SeNPs) for the treatment of post-surgical wounds in children; to evaluate antimicrobial properties, healing, and biocompatibility through in vitro and in vivo tests |
| Luo et al. (2022) | China | Clinical evaluation of dressings with silver nanoparticles | To evaluate the efficacy of dressings with nanostructured silver ions in the treatment of infected surgical wounds; to compare the antimicrobial action of silver nanoparticle dressings (Ag-PVP NPs) with conventional antibiotics; to investigate the impact of the use of these dressings in reducing the risk of infection and healing time |
| Lu et al. (2022) | China | Synthesis and characterization of nanoparticles, antimicrobial and healing evaluation in vitro | To develop an antimicrobial dressing based on sustainably synthesized silver nanoparticles (AgNPs) for application in surgical wounds after rectal surgery; to evaluate the antimicrobial properties, bioactivity, and healing capacity of AgNPs in comparison to the plant extract used in the synthesis |
Main Articles on Biomaterials and Dressings Combined with Nanotechnology for Wound Treatment
Smart Dressings
Smart dressings, also known as intelligent dressings, are designed to incorporate sensors and technologies to monitor the physiological parameters of the wound bed in real time (Jiang; Loo, 2021; Deng et al., 2025; Moradifar et al., 2025). These devices are designed to detect critical factors, such as pH, reactive oxygen species, specific enzymes, glucose levels, light, heat, and temperature, allowing for more precise and personalized interventions (Alberts et al., 2025; Deng et al., 2025; Zhang et al., 2025). In addition, many innovative dressings are responsive, releasing therapeutic agents, such as antibiotics, in a controlled manner in response to specific wound conditions (Jiang; Loo, 2021). One example is pH-responsive dressings. The normal pH of the skin ranges from 5 to 6; however, in wounds colonized by microorganisms, the pH can range from 7 to 10. Thus, smart dressings that respond to pH stimuli will release their antimicrobials when the pH level increases, thereby controlling microbial proliferation in a personalized manner (Alberts et al., 2025). These dressings can respond to one or more stimuli (Jiang; Loo, 2021). They have been increasingly researched and have shown promising results. In vitro and in vivo studies have demonstrated that a smart hydrogel, combining materials such as gelatin and chitosan methacrylate, nanoparticles, and a pH indicator, can be analyzed using machine learning and is an efficient, regenerative, biocompatible, bioactive, antibacterial, and anti-inflammatory product (Deng et al., 2025). In China, a chitosan-based dressing incorporates smart sensors to monitor wound temperature and humidity in real time, enabling rapid responses from medical staff (Yang et al., 2023). These are some results from applying various technologies to the development of new dressings.
Bioactive Dressings
Bioactive dressings are designed to interact actively with the wound bed, releasing bioactive compounds that modulate inflammation, stimulate cell proliferation, promote angiogenesis, and accelerate tissue regeneration (He et al., 2023). These dressings are developed from natural or synthetic matrices, often incorporated with biological agents, such as natural extracts, nanoparticles, growth factors, or even cells, thus optimizing the healing microenvironment (Maxson et al., 2012; He et al., 2023). In this context, researchers have extensively studied natural compounds, such as chitosan, collagen, and cellulose, in the development of bioactive dressings. Nanotechnology has also played a pivotal role in this field, enabling the controlled release of bio-active agents and enhancing their therapeutic efficacy (Dhivya et al., 2015). Another study reports that a hydrogel based on polyhydroxyethyl methacrylate (PHEM) and chitosan (CS), incorporated with cerium oxide nanoparticles (CeONPs), showed antimicrobial properties, biocompatibility, and accelerated healing in chronic wounds (Luo et al., 2023). Other examples are bioactive dressings based on medicinal plant extracts. Studies reveal that electrospun nanofibrous dressings coupled with plant extracts represent an essential alternative for treating wounds, owing to their efficiency, the high availability of plant material, costeffectiveness, and environmental compatibility (Adamu et al., 2021). These reports demonstrate how bioactive dressings integrate materials engineering and biotechnology to provide highly effective therapeutic solutions. Thus, these dressings represent a promising and innovative approach, particularly for treating difficult-to-heal wounds.
3D-Printed Dressings
3D-printed dressings represent one of the most significant advances in bioengineering applied to wound treatment. This technology enables the manufacture of personalized dressings tailored to the exact dimensions of the lesion and the patient’s anatomical shape (Leppiniemi et al., 2017; Yayehrad et al., 2023; Astaneh & Fereydouni, 2024). These dressings are generally manufactured from biopolymers such as methacrylated gelatin, chitosan, hyaluronic acid, and nanocellulose, often combined with therapeutic agents, such as antimicrobials, growth factors, nanoparticles, or living cells (Leppiniemi et al., 2017; Boateng et al., 2023; Yayehrad et al., 2023; Astaneh; Fereydouni, 2024; Rossi et al., 2024). Studies on this technology have been conducted with increasing frequency in recent years. A bioactivated nanocellulose-alginate hydrogel showed excellent structural stability after 3D printing, maintaining its shape and mechanical properties (Leppiniemi et al. 2017). Additionally, the material exhibited tunable mechanical properties and good moisture retention, which are essential characteristics for applications in wound dressings and tissue engineering.
Another study reports that a methacrylated gelatin hydrogel incorporating lignin-derived carbon dots was evaluated for its antimicrobial properties in the development of a 3D-printed dressing. The results demonstrated that the dressing has effective antimicrobial activity against Staphylococcus aureus and Escherichia coli and does not present cytotoxicity in human fibroblasts. The material also maintained a hydrated environment in the wound area, a crucial factor for optimal healing (Rossi et al., 2024). Growth factors are also associated with 3D printing technology and have shown promising results for application in these dressings, with a relatively long release profile (Boateng et al., 2023). Other studies report the integration of silver nanoparticles with 3D printing technology to develop dressings, demonstrating promising results (Astaneh and Fereydouni, 2024). However, these authors also note challenges in nanoparticle applications within 3D structures, including the uniform dispersion of these nanomaterials and the potential cytotoxicity at high concentrations. 3D-printed dressings, therefore, offer an innovative and personalized solution in treating wounds. Their ability to combine biomaterials, bioactive agents, and adaptable design makes this technology promising for regenerative medicine.
Sustainability and Development of New Dressings
Sustainable development in wound dressings has become an urgent issue, given the environmental impacts associated with their production, use, and disposal. Among the concerning data on waste generated in the healthcare system, materials used to treat wounds are a significant portion of this waste, originating from dental and veterinary clinics, offices, medical departments, and other sources (Janik-Karpinska et al., 2023). In addition, many dressings have traditionally included synthetic polymers derived from petroleum, such as polyurethane, in part of their composition (Sood et al. 2014; Nguyen et al., 2023; Zhang et al., 2024). These materials have low biodegradability and generate persistent waste in the environment. The inadequate disposal of these materials, coupled with their greater permanence in the environment, not only contributes to the generation of solid waste but also carries biological and chemical contaminants, thereby increasing health and environmental risks (Borowy, 2020).
Given this scenario, there is growing interest in sustainable alternatives for manufacturing dressings. The use of natural biopolymers, such as chitosan, bacterial cellulose, collagen, hyaluronic acid, and fibrin, has been highlighted due to their biodegradability, biocompatibility, and often intrinsic antimicrobial properties (Leppiniemi et al., 2017; Boateng et al., 2023; Nguyen et al., 2023; Yang et al., 2023; Yayehrad et al., 2023; Astaneh; Fereydouni, 2024; Rossi et al., 2024). These characteristics can help reduce environmental damage and contamination caused by the accumulation of waste resulting from wound treatment. Another sustainable strategy is to use industrial waste to formulate biomaterials. Lignin, for example, has been increasingly investigated for application in wound dressings due to its adhesive, antibacterial, and antifungal properties, and has shown promising results even in more advanced technologies such as 3D printing dressings (Domínguez-Robles et al., 2023; Rossi et al., 2024; Wan et al., 2024).
Research shows that approximately 10 million tons of lignin are generated as a byproduct of paper and ethanol production (Bajwa et al., 2019). Using this bioproduct in the development of dressings could be a sustainable alternative. Another example of a byproduct is cellulose, which can be extracted from lignocellulosic waste from paper production (Souza et al., 2017), and the wood vinegar generated during the wood carbonization process for charcoal production (Gama et al., 2023). In addition to these examples, several other promising bioproducts can be found as byproducts from various production processes. Incorporating them into the production of biodegradable and efficient dressings qualifies as an alternative to make wound treatment more sustainable.
Limitations and Future Prospects
Despite significant advances in wound dressing science and adjunctive therapies, wound care continues to face substantial challenges. Essential limitations include the lack of in vivo testing, human clinical trials, long-term evaluations, skilled labor, costs, and potential regulatory challenges (Laurano et al., 2022; Luo et al., 2023; Ruan et al., 2023; Yang et al., 2023; Namgoong et al., 2023; Liu et al., 2024). A study conducted in South Korea demonstrated that skilled labor in handling dressings improves care performance, patient and healthcare professional satisfaction, and yields more satisfactory wound care outcomes (Namgoong et al., 2023). These findings demonstrate that, even in large centers, the introduction of advanced dressings requires trained professionals and specific protocols, and that the absence of these results in inadequate application increases the risk of complications and inferior clinical outcomes. The lack of in vivo testing and clinical trials in humans is also a limitation to the implementation of new technologies for the practical treatment of wounds, as it generates a lack of robust evidence of the efficacy and safety of the products being developed (Ruan et al., 2023; Yang et al., 2023; Liu et al., 2024). In other words, dressings that work well in vitro may fail in vivo due to the complexity of the human biological environment, including enzymes, microbiota, the immune system, and blood flow, which can compromise their effectiveness. Another limitation reported in the research is the lack of long-term evaluations (Luo et al., 2022; Ruan et al., 2023; Luo et al., 2023; Yang et al., 2023).
This scenario raises uncertainty about the durability of therapeutic effects, as without long-term follow-up studies, it is challenging to determine whether the benefits observed in the early stages of healing are sustained over time. The high costs of developing and producing more technologically advanced dressings also pose a significant limitation to their implementation in wound treatment (Luo et al., 2022; Laurano et al., 2022; Ruan et al., 2023). These costs are reflected in higher hospital and patient prices, making it difficult for them to be incorporated on a large scale into public health systems. Additionally, regulatory processes make it highly challenging for advanced dressings to enter the market quickly (Laurano et al., 2022). Therefore, these limitations compromise the widespread implementation of new dressings in the health system. These challenges delay patients’ access to more effective therapies and impede scientific and technological innovation in wound healing. Overcoming them ensures more advanced, safe, and sustainable treatments.
Prospects for wound treatment point to the development of multifunctional smart dressings capable of continuously monitoring the wound microenvironment and releasing therapeutic agents in a controlled manner, responsive to specific stimuli such as pH, temperature or the presence of infections (Alberts et al., 2025; Jiang; Loo, 2021; Deng et al., 2025; Moradifar et al., 2025; Zhang et al., 2025). The integration of technologies such as nanotechnology and 3D printing allows the creation of personalized devices that are adaptable to the individual characteristics of each patient, optimizing therapeutic results (Leppiniemi et al., 2017; Adamu et al., 2021; He et al., 2023; Yayehrad et al., 2023; Astaneh; Fereydouni, 2024; Deng et al., 2025). Furthermore, advances in bioengineering, for example, have driven the use of stem cells, growth factors, and bioactive scaffolds for tissue regeneration, which could revolutionize the treatment of chronic and complex wounds (Yamakawa; Hayashida, 2019; Riedl et al., 2021; Sierra-Sánchez et al., 2021; Han et al., 2022; Downer et al., 2023; Soriano et al., 2023; Ferreira et al., 2024). However, for these innovations to become accessible clinical practices, it is essential to overcome regulatory challenges, reduce production costs, expand clinical studies with long-term follow-up, and train professionals to handle them.
Conclusion
Wound treatment represents one of the most significant challenges in modern medicine, especially given the increasing complexity of skin lesions. Choosing the appropriate dressing based on the characteristics of the wound (such as exudate, depth, and infection status) is crucial for therapeutic success. This work has highlighted the wide range of dressings, from traditional and conventional approaches (gauze, tulles, adhesive tapes) to high-technology systems (bioactive, smart, nanotechnological, and 3D-printed dressings).
Although conventional dressings remain useful in clinical practice, advanced dressings offer innovative solutions that extend beyond simple protection, such as real-time monitoring of clinical parameters and the controlled release of therapeutic agents. Furthermore, adjunctive therapies, including stem cells, growth factors, and non-thermal plasma, provide a multitherapeutic approach that significantly improves the healing of chronic and complex wounds. Despite promising prospects, challenges such as high costs, limited clinical validation, and environmental impacts still need to be addressed. Sustainable development in dressing production, including the use of natural biopolymers and industrial byproducts, is an emerging field that promises to reconcile clinical efficacy with environmental responsibility.
In conclusion, the evolution of wound dressings and adjunctive therapies reflects a continuous search for more efficient, personalized, and sustainable solutions. Collaboration between different fields of knowledge, such as materials engineering, biology, nursing, and medical care, is essential to consolidate these innovations and ensure their effective implementation in global wound care practice.
AI or AI-assisted tools were not used in drafting or final writing of this manuscript.
We thank the Brazilian Coordination for the Improvement of Higher Education Personnel (CAPES) and the National Council for Scientific and Technological Development (CNPq) for research funding, graduate scholarships, and support for researchers.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
Funding
This work did not receive any external funding.
References
Cite this article
Related Research

Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.


