Provide your details below to request scholarly review comments.
×
Verified Request System ®
Order Article Reprints
Please fill in the form below to order high-quality article reprints.
×
Scholarly Reprints Division ®
− Abstract
Pelvic bone cancer is a serious medical condition that often remains undetected in its early stages due to non-specific symptoms and the complex anatomical structure of the pelvic region. Common clinical symptoms include persistent pelvic pain, swelling, restricted movement, unexplained weight loss, and fatigue, which are frequently mistaken for musculoskeletal disorders. Factors such as genetic predisposition, previous radiation exposure, bone disorders, and long-term inflammation are considered significant contributors to the development of pelvic bone malignancies. Delayed diagnosis increases disease severity, highlighting the importance of early detection and public awareness. Magnetic Resonance Imaging (MRI) plays a vital role in visualising pelvic bone abnormalities due to its superior soft-tissue contrast. This study proposes an automated framework for pelvic bone cancer detection that integrates image filtering, region extraction, and clustering-based segmentation. During preprocessing, median filtering and Gaussian filtering are applied to MRI images to suppress noise, smooth intensity variations, and enhance structural visibility. This filtering stage improves image quality and supports accurate identification of abnormal tissue regions. A Region of Interest (ROI) extraction step then isolates tumour-suspected pelvic areas, reducing interference from surrounding tissues. The extracted ROIs are segmented using K-means clustering and Fuzzy C-Means (FCM) algorithms based on intensity and spatial characteristics. While K-means performs hard clustering, FCM enables soft classification through membership values, resulting in improved tumour boundary delineation in complex pelvic structures. Experimental results show that FCM outperforms K-means in handling overlapping tissue intensities. This automated, filtering-assisted approach can serve as a supportive diagnostic tool for radiologists. Moreover, the study emphasises the importance of early symptom recognition and timely medical consultation to reduce fear, increase awareness, and improve survival outcomes among individuals at risk of pelvic bone cancer.
− Explore Digital Article Text
# I. INTRODUCTION
Pelvic bone cancer is a rare but aggressive form of malignancy that affects the bony structures of the pelvic region, including the ilium, ischium, pubis, and sacrum. These tumours may arise as primary bone cancers or occur as secondary lesions due to metastatic spread from cancers of other organs, such as the prostate, breast, lung, or kidney. The deep anatomical location of the pelvis, combined with the proximity of vital organs and neurovascular structures, makes early diagnosis particularly challenging. Consequently, pelvic bone cancers are often detected at advanced stages, leading to limited treatment options and reduced survival rates.
# 1.1 Normal Versus Malignant Pelvic Bone Conditions
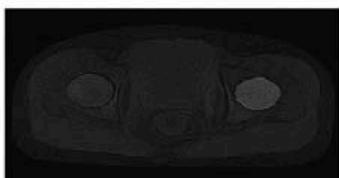
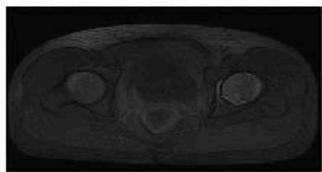
Under normal physiological conditions, pelvic bones maintain structural stability through regulated cellular growth and continuous bone remodelling. Healthy bone tissue demonstrates balanced metabolic activity, uniform density, and clearly defined anatomical margins. Imaging studies of normal pelvic bones typically reveal consistent signal intensities and intact cortical structures without abnormal tissue formation. In malignant conditions, this controlled cellular process is disrupted, resulting in uncontrolled proliferation of abnormal cells. Cancerous growth leads to destruction of healthy bone, irregular tissue architecture, and possible invasion of surrounding soft tissues. Malignant pelvic bone tumours often present with heterogeneous imaging characteristics, including irregular margins, altered marrow signals, and associated soft-tissue masses. These pathological changes may progress significantly before clinical symptoms become evident, further complicating early diagnosis.
# 1.2 Clinical Symptoms and Risk Factors
The clinical presentation of pelvic bone cancer is often non-specific, which contributes to delayed diagnosis. Persistent pelvic or hip pain is the most common symptom and typically worsens over time. Additional symptoms may include localised swelling, stiffness, reduced mobility, and difficulty performing daily activities such as walking or sitting. In advanced stages, patients may experience pathological fractures due to bone weakening, as well as systemic symptoms such as fatigue, unexplained weight loss, fever, and night pain. Neurological symptoms may arise when tumours compress nearby nerves or spinal structures. Several factors have been associated with an increased risk of developing pelvic bone cancer. These include genetic predisposition, inherited cancer syndromes, previous exposure to high-dose radiation therapy, and certain pre-existing bone disorders. Age also plays a significant role, as some tumour types are more prevalent in younger individuals, while others occur more frequently in older populations. Metastatic involvement of pelvic bones is commonly observed in patients with advanced-stage cancers originating from other organs.
# 1.3 Treatment Strategies and Patient Care
The management of pelvic bone cancer requires a multidisciplinary approach tailored to the tumour type, stage, and patient health status. Surgical resection is often the primary treatment option when complete tumour removal is feasible. Radiotherapy may be used as an adjunct treatment or as a palliative measure to control tumour growth and relieve pain. Chemotherapy is commonly administered for aggressive tumours, particularly in pediatric and young adult patients, to eliminate rapidly dividing cancer cells and reduce the risk of metastasis. In addition to these primary treatments, supportive medications such as pain relievers, anti-inflammatory drugs, and bone-strengthening agents are routinely prescribed to improve patient comfort and quality of life. Emerging treatment options, including targeted therapy and immunotherapy, offer promising outcomes with fewer side effects. Patient care typically involves diagnosis, staging, treatment planning, therapeutic intervention, rehabilitation, and long-term follow-up, with psychological and physical support playing a crucial role throughout the treatment process.
# 1.4 Role of Medical Imaging and Machine Learning
Medical imaging is fundamental to the detection and evaluation of pelvic bone cancer. Among available imaging modalities, Magnetic Resonance Imaging (MRI) is particularly valuable due to its superior soft-tissue contrast and ability to visualise bone marrow abnormalities. However, manual interpretation of MRI scans is time-consuming and subject to observer variability. Recent advances in machine learning have introduced powerful tools for automated medical image analysis. Machine learning algorithms can learn complex patterns from imaging data and assist in differentiating normal tissue from malignant lesions. In this research, machine learning techniques are applied to MRI images to support automated pelvic bone cancer detection. Image preprocessing and feature extraction enhance data quality, while clustering and classification algorithms such as K-means and Fuzzy C-Means enable accurate segmentation of tumour regions. The integration of machine learning into diagnostic workflows has the potential to improve early detection, reduce diagnostic errors, and support clinical decision-making.
# 1.5 Importance of Awareness and Early Detection
Increasing public and clinical awareness of pelvic bone cancer symptoms is essential for promoting early diagnosis and effective treatment. Persistent pelvic pain, unexplained swelling, and functional limitations should prompt a timely medical evaluation. The combined use of advanced imaging techniques and machine learning-based diagnostic systems offers significant potential to improve early detection rates, enhance treatment outcomes, and reduce the overall burden of pelvic bone cancer.
# II. LITERATURE REVIEW
Pelvic bone cancer represents one of the most challenging musculoskeletal malignancies to diagnose and manage due to its deep anatomical location and complex structural composition. The pelvic region consists of multiple bones, joints, and surrounding organs, which often obscure early pathological changes. Previous clinical studies have reported that pelvic bone tumours frequently present with non-specific symptoms, such as persistent pain or reduced mobility, which are commonly misinterpreted as benign musculoskeletal conditions. As a result, diagnosis is often delayed until the disease reaches an advanced stage, negatively affecting treatment outcomes and patient survival (Bielack et al., 2002).
Clinical investigations have shown that pelvic bone malignancies include a range of tumour types, such as osteosarcoma, chondrosarcoma, and Ewing's sarcoma. These tumours demonstrate aggressive biological behaviour and a high potential for local invasion. Damron et al. (2007) emphasised that tumours located in the pelvic region are associated with poorer prognostic outcomes compared to tumours of the extremities, primarily due to difficulties in early detection and complete surgical resection. The proximity of pelvic bones to vital neurovascular structures further complicates both diagnosis and treatment planning.
Medical imaging has therefore become a cornerstone in the evaluation of pelvic bone cancer. Conventional radiographic techniques provide limited diagnostic information due to overlapping anatomical structures and insufficient soft-tissue contrast. Advanced imaging modalities, particularly Magnetic Resonance Imaging (MRI), offer superior visualisation of bone marrow abnormalities and soft tissue involvement. MRI enables clinicians to assess tumour extent, internal composition, and surrounding tissue invasion with greater accuracy (Chowdhry et al., 2014). Despite these advantages, MRI interpretation remains highly dependent on radiologist expertise and is subject to inter-observer variability.
To overcome these limitations, researchers have increasingly focused on computational methods for automated medical image analysis. Image preprocessing techniques play a crucial role in enhancing image quality and improving diagnostic reliability. Filtering methods such as median filtering have been shown to effectively remove impulse noise while preserving important structural edges, whereas Gaussian filtering smooths intensity variations and enhances contrast (Greenspan et al., 2015). These techniques are widely used in musculoskeletal imaging to prepare data for subsequent analysis stages.
In addition to preprocessing, isolating relevant anatomical regions has been shown to improve diagnostic accuracy. Region-based analysis allows computational models to focus on suspected pathological areas while reducing the influence of irrelevant background information. In pelvic imaging, this approach is particularly valuable due to the presence of surrounding organs and complex skeletal geometry. Several studies have demonstrated that region-focused analysis improves segmentation precision and computational efficiency in bone tumour detection (Fletcher et al., 2013).
Machine learning techniques have gained considerable attention in recent years for their ability to analyse complex medical imaging data. Unsupervised learning methods are especially useful in medical applications where labelled datasets are limited. Clustering algorithms group image pixels based on similarity measures such as intensity and spatial characteristics, making them suitable for tumour segmentation tasks. K-means clustering has been widely applied due to its simplicity and computational efficiency; however, its reliance on hard clustering limits its ability to accurately segment regions with overlapping tissue intensities (Pham et al., 2000).
Fuzzy C-Means (FCM) clustering has been proposed as an effective alternative for medical image segmentation. Unlike K-means, FCM assigns membership values to pixels, allowing them to belong to multiple clusters simultaneously. This soft clustering approach has been shown to produce smoother and more accurate segmentation results, particularly in heterogeneous tissues such as bone and marrow regions. Multiple studies have reported improved boundary detection and reduced misclassification when FCM is applied to tumour segmentation problems (Bezdek et al., 1984).
The integration of machine learning into medical imaging has led to the development of computer-aided diagnosis systems that support clinicians in detecting and evaluating cancerous lesions. These systems aim to enhance diagnostic consistency, reduce human error, and assist radiologists in handling large volumes of imaging data. Litjens et al. (2017) demonstrated that machine learning-based systems significantly improve performance in various medical image analysis tasks, including segmentation and classification. In the context of pelvic bone cancer, automated image analysis systems provide valuable support by enabling early identification of malignant regions and facilitating accurate treatment planning. By combining advanced imaging techniques with machine learning algorithms, these systems contribute to improved diagnostic accuracy and better patient management. The continued development of such approaches highlights the growing importance of computational intelligence in modern oncological imaging.
# III. METHODOLOGY
This research employs a systematic and image-based machine learning approach to detect pelvic bone cancer using Magnetic Resonance Imaging (MRI) data. The MRI images used in this study were collected from several hospitals and diagnostic imaging centres located in Tamil Nadu, India. All images were obtained following standard clinical protocols and were anonymised to ensure patient confidentiality. The dataset includes both cancer-affected and non-cancer pelvic MRI scans, enabling reliable comparative analysis. Images from both male and female patients were included, covering a wide age range, starting from pediatric patients aged five years to elderly patients aged seventy five years and above. This diverse demographic distribution ensures that the proposed system is robust and applicable across different age groups and genders. The collected MRI dataset represents a variety of pelvic bone conditions. Normal pelvic images exhibit uniform bone structure and consistent signal intensity, whereas malignant images show irregular tissue patterns, altered intensity distributions, and structural disruptions caused by abnormal cell growth. Before analysis, all images were standardised in terms of size and format to maintain consistency throughout the processing pipeline. This normalisation step ensures that the subsequent image processing and machine learning algorithms perform reliably across the entire dataset.
Image preprocessing was carried out to enhance image quality and suppress noise inherent in MRI acquisition. Initially, a mean filtering technique was applied to reduce random noise by averaging pixel intensities within a local neighbourhood. This process improves image smoothness and removes minor intensity variations. Following this, Gaussian filtering was employed to further smooth the images while preserving essential anatomical boundaries. The Gaussian filter
reduces high-frequency noise and enhances contrast between normal and abnormal pelvic bone tissues, thereby improving the visibility of potential cancer regions. After preprocessing, a Region of Interest (ROI) extraction method was applied to isolate pelvic bone regions that were suspected of containing cancerous tissue. The ROI extraction process limits the analysis to relevant anatomical areas and minimises the influence of surrounding organs and background structures. By focusing on the pelvic bone region, this step improves segmentation accuracy and reduces computational complexity, allowing the machine learning algorithms to concentrate on clinically significant regions.
To identify and segment pelvic cancer regions, two unsupervised machine learning algorithms were applied: K-means clustering and Fuzzy C-Means (FCM) clustering. K-means clustering groups image pixels into distinct clusters based on similarity in intensity values and spatial characteristics. Due to its simplicity and computational efficiency, K-means is effective for initial segmentation; however, its hard clustering nature restricts each pixel to a single cluster, which can limit accuracy in areas where tissue intensities overlap. In contrast, Fuzzy C-Means clustering assigns membership values to each pixel, allowing pixels to belong to multiple clusters simultaneously. This soft clustering approach is particularly suitable for medical images, where tumour boundaries are often unclear, and tissue characteristics vary gradually. Following segmentation, the clustered output images were analysed to detect cancer-affected regions. Malignant pelvic bone regions were identified based on irregular shapes, heterogeneous intensity distributions, and discontinuities in bone structure. These characteristics were compared with normal pelvic bone features to distinguish cancerous tissue from healthy regions. The segmentation results produced by both algorithms were evaluated through quantitative measures and expert visual assessment to determine their effectiveness. A comparative analysis was conducted to assess the performance of K-means and Fuzzy C-Means algorithms in pelvic cancer region detection.
While K-means demonstrated faster execution time, Fuzzy C-Means consistently produced smoother and more accurate segmentation results, particularly in cases involving overlapping tissue intensities and complex pelvic structures.
Based on the experimental findings, Fuzzy C-Means was identified as the more reliable algorithm for precise pelvic bone cancer detection in MRI images. Overall, the proposed methodology integrates clinically sourced MRI data, effective preprocessing techniques, ROI extraction, and machine learning-based segmentation to support automated pelvic bone cancer detection. The inclusion of diverse patient demographics and comparative algorithm analysis enhances the clinical relevance and reliability of the proposed approach.
# METHODOLOGY
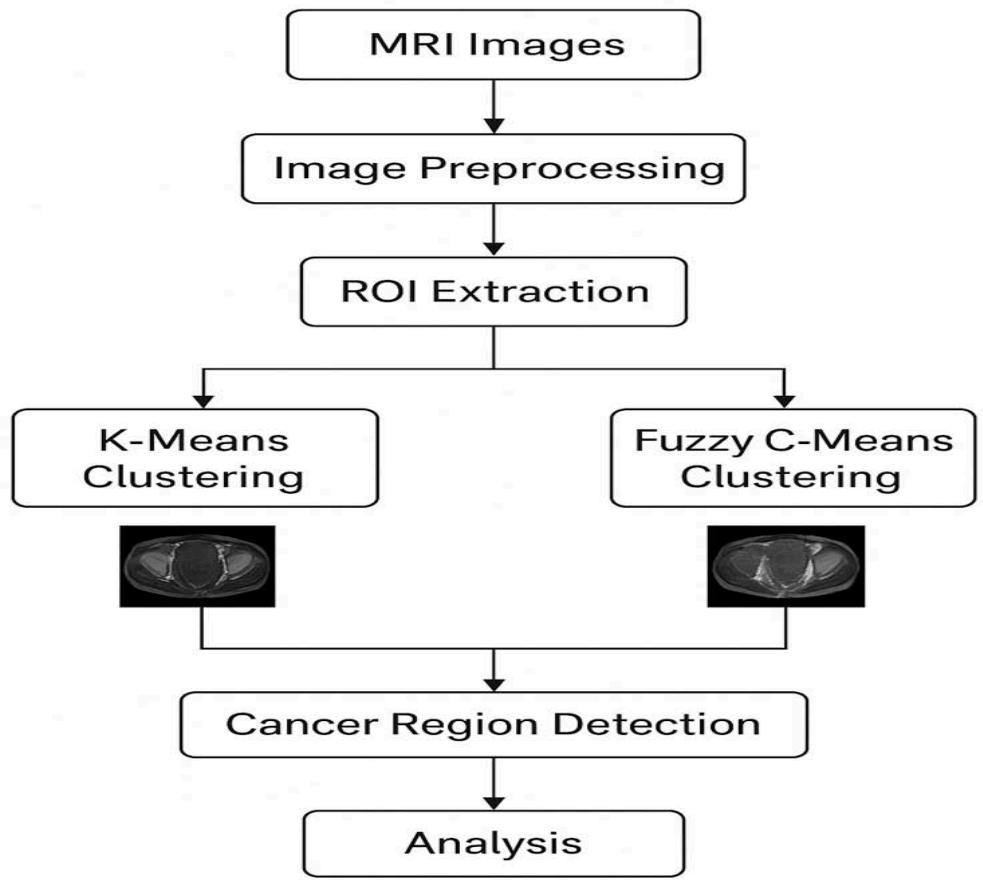
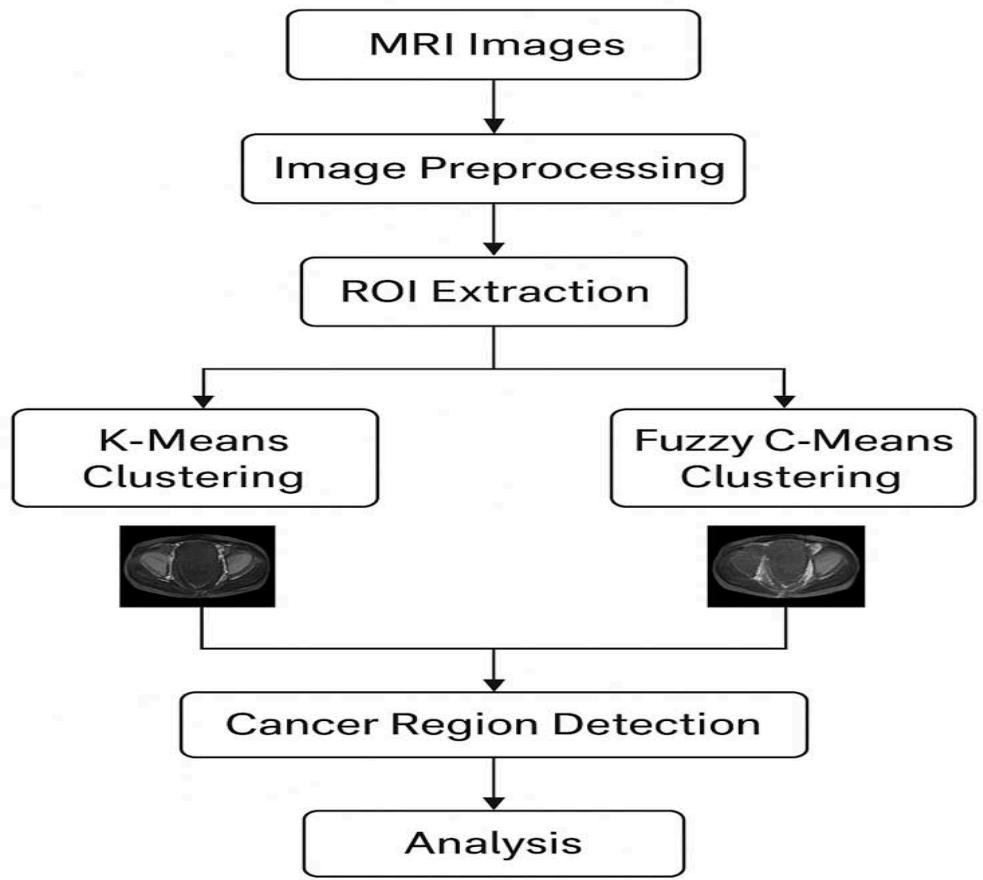
Figure 1: Diagram of the pelvic cancer detection research flow structure
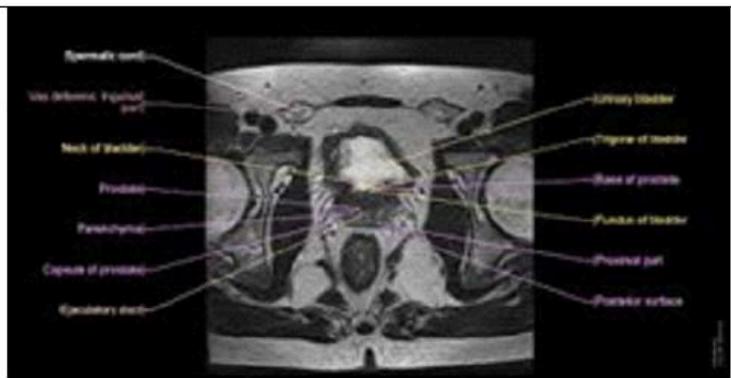
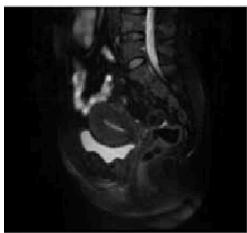
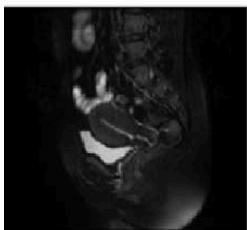
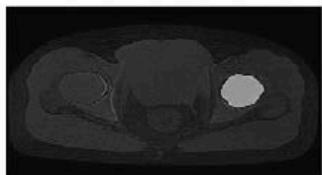
# Normal
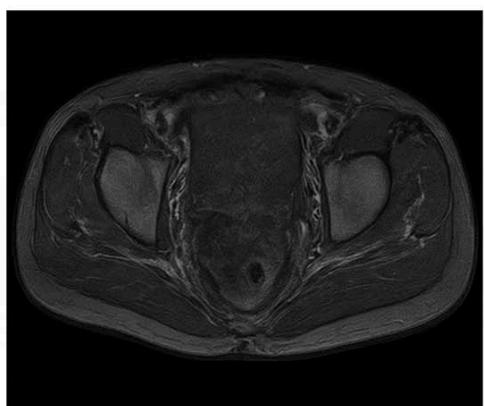
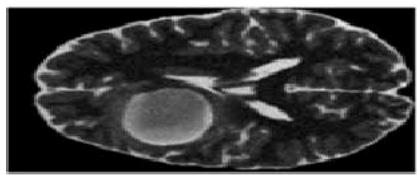
Figure 2: The Sample of Pelvic Cancer and Normal in MRI Scan Images
# Cancer
# IV. RESULTS AND DISCUSSION
The experimental results obtained from the proposed pelvic bone cancer detection framework demonstrate the effectiveness of each processing stage applied to MRI images. The original input MRI images provided clear anatomical information of the pelvic region; however, noise and intensity variations limited direct identification of abnormal tissues. After applying preprocessing techniques such as median filtering and contrast enhancement, the visual clarity of the images improved noticeably. Noise artifacts were reduced, and structural details of bone and surrounding tissues became more distinguishable, enabling reliable further analysis.
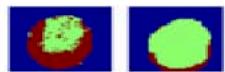
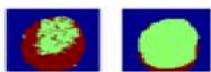
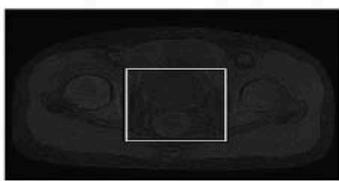
The extraction of the Region of Interest (ROI) played a significant role in isolating the pelvic bone area by eliminating irrelevant background information. This step ensured that only clinically meaningful regions were considered during segmentation, thereby improving detection accuracy and reducing computational complexity. The ROI images showed enhanced focus on suspected abnormal regions, supporting effective clustering-based segmentation. K-Means clustering segmented the ROI into distinct intensity-based regions, allowing the suspected cancer area to be identified as a separate high-intensity cluster. Although the method provided fast and clear segmentation, minor inaccuracies were observed at tissue boundaries due to its hard clustering mechanism. In contrast, Fuzzy C-Means clustering produced smoother and more accurate segmentation results by assigning partial membership values to pixels. This approach was particularly effective in preserving tumor boundaries and handling intensity overlaps between healthy and affected tissues.
1. Input MRI Images

Figure 2a: Shows in MRI Pelvic Cancer Images

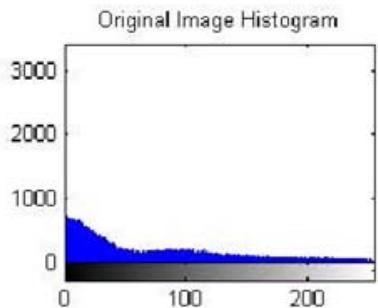

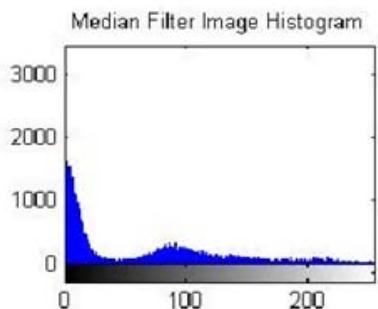

Figure 3: The Shows the Result in Preprocessed Mri Output
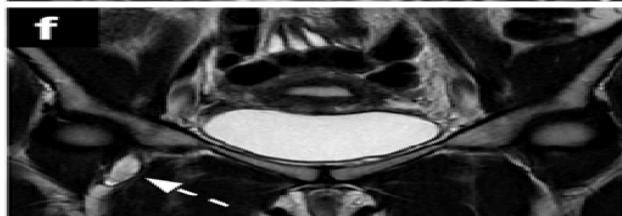
(a) Original Image


(b) Uterine Region Detection Image
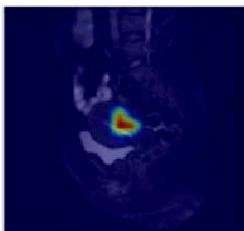
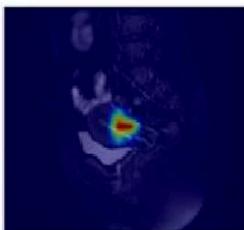
(c) CAM image
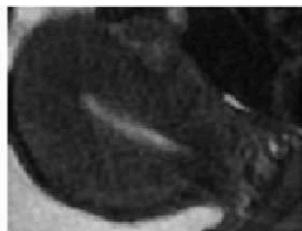
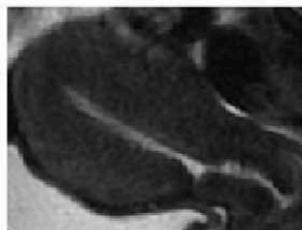
(d) Uterine Region Save Crop
(e) Prediction Visualization
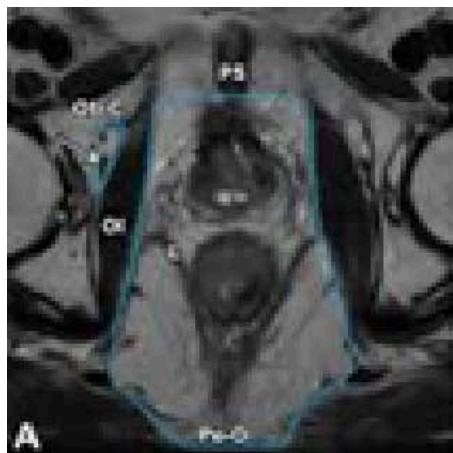
Figure 4: The Result is Shown in the Roi Extraction Result
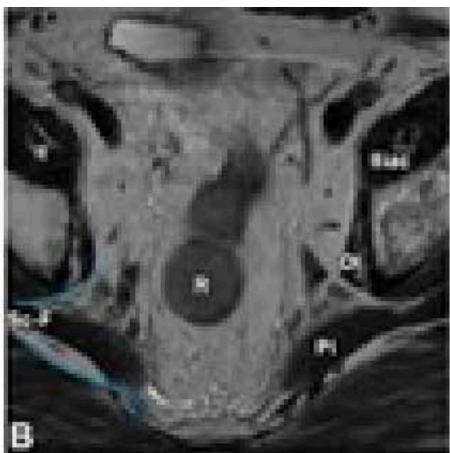
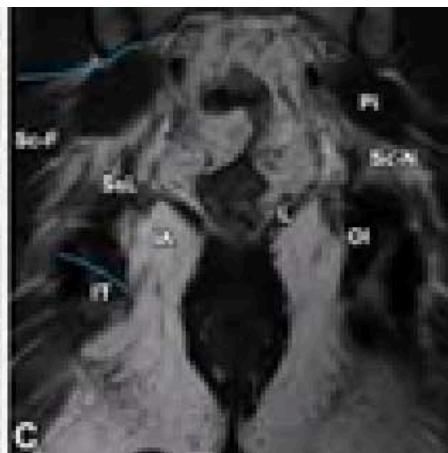
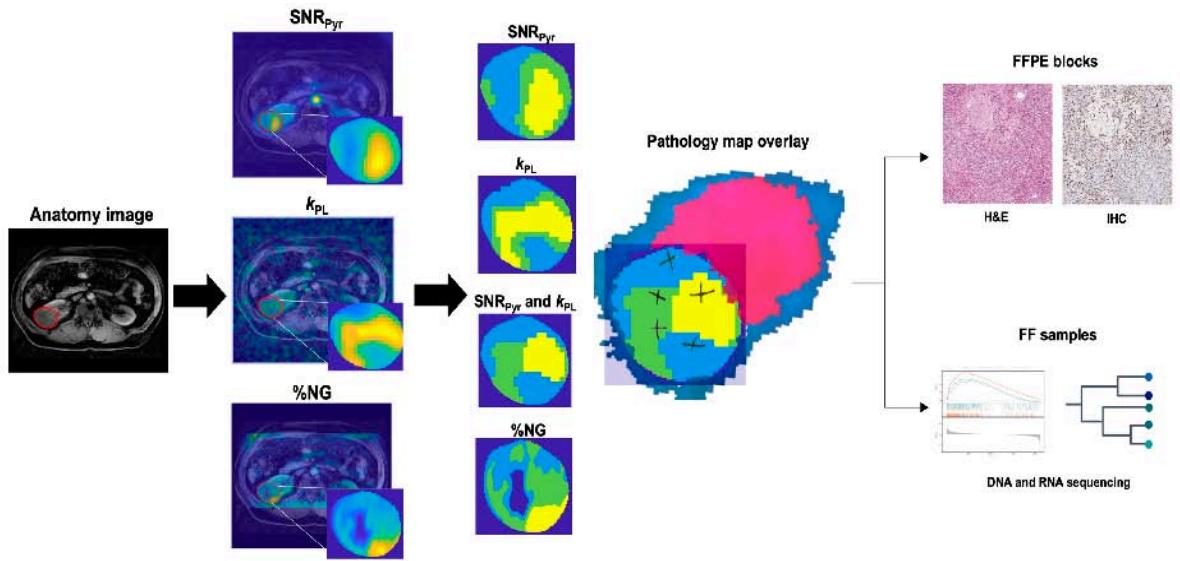
Figure 5: The Result Shows in K-Means Clustering Output of Anatomy to Pathological Overview
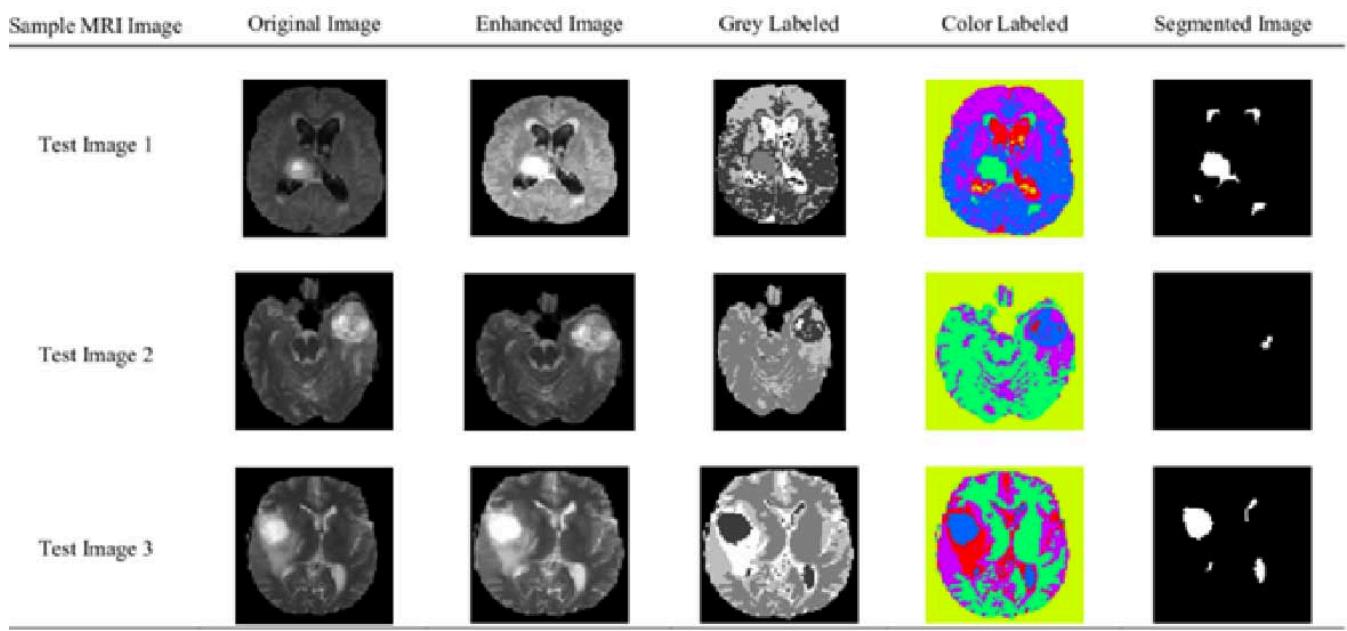
Figure 5a: The Result Shows in K-Means Clustering Output

(a)

(b)

(c)

(d)

(e)

(f)

(g)
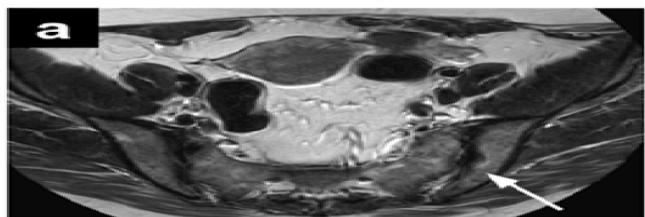
Figure 6: The Result Shows in Fuzzy C-Means Clustering Output
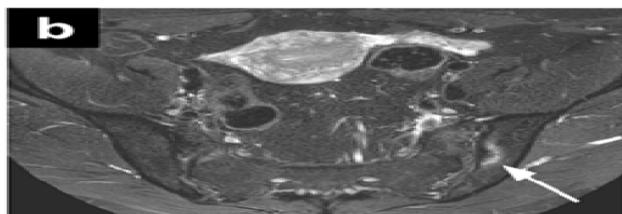
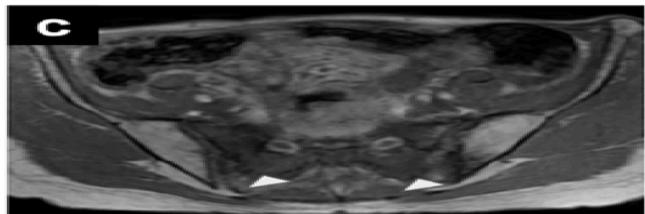
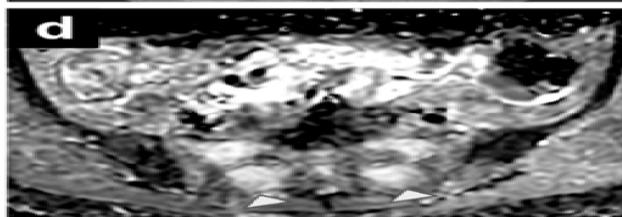
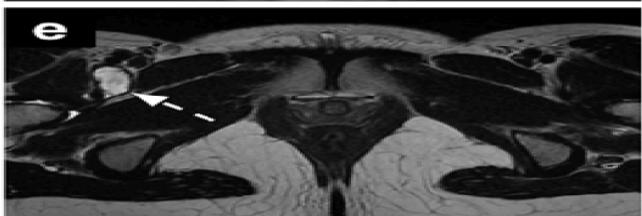
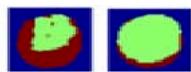
Figure 6a: The Result Shows in Final Cancer Region Detection
# RESULTS
Input MRI Images
ROI Extraction
Fuzzy C-Means Clustering
Preprocessed MRI Output
K-Means Clustering

Final Cancer Region Detection
Figure 6b: The Result Shows the Pelvic Cancer Detection
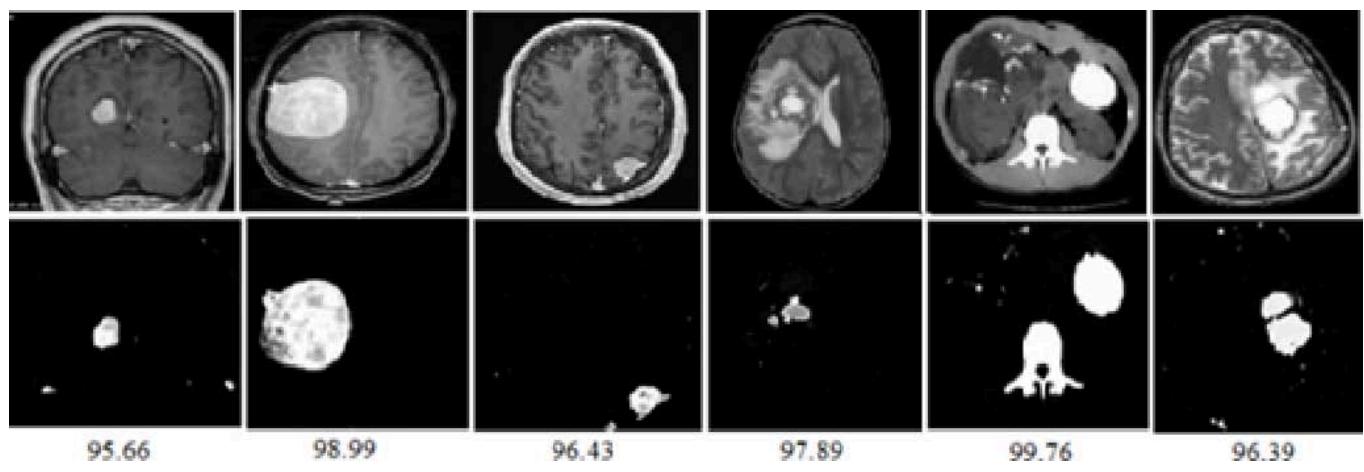
The final cancer region detection output clearly highlighted the abnormal regions within the pelvic bone. The detected areas closely corresponded with visually observed irregularities in the MRI images, confirming the reliability of the proposed method. The comparative results indicate that while both clustering techniques are effective, Fuzzy C-Means offers superior performance for medical image segmentation due to its flexibility and boundary preservation capability. Overall, the results validate that the proposed MRI-based framework can serve as a supportive diagnostic tool for early and accurate pelvic bone cancer detection.
# V. CONCLUSION
The proposed MRI-based framework for pelvic bone cancer detection demonstrates effective performance through a structured sequence of preprocessing, region extraction, and clustering-based segmentation. By enhancing image quality and isolating relevant anatomical regions, the system successfully reduces noise and background interference, which are common challenges in medical image analysis. The extracted regions of interest allow focused examination of pelvic bone structures, leading to more reliable identification of abnormal tissue patterns. The comparative evaluation of K-Means and Fuzzy C-Means clustering highlights the importance of soft clustering techniques in medical imaging applications. While K-Means offers faster segmentation, Fuzzy C-Means provides improved boundary accuracy and better representation of complex tissue transitions. The final detection results confirm that the proposed approach can effectively distinguish cancer-affected regions from healthy pelvic bone tissue in MRI images. Overall, the experimental outcomes validate that the developed framework is capable of assisting clinical decision-making by providing a non-invasive and automated support tool for pelvic bone cancer detection. The methodology shows strong potential for early diagnosis and can be further enhanced by integrating advanced feature extraction methods and deep learning models in future work to improve accuracy and robustness across larger and more diverse datasets.
# Authors' Assent and Recognition:
1. Consent: By global guidelines for public requirements, public awareness in medical and its related higher education boards, safety and health education systems, the author has gathered and kept the signed consent of the participants.
2. Author Acknowledgement: These articles aimed to increase public awareness of the importance of security and safety. Sources that illustrate development and security are drawn from the relevant database to support the study's objectives. Don't make any assertions about readers, viewers, or authorities.
3. Approvals for Ethics: The authors hereby declare that all experiments have been reviewed and approved by the relevant ethics bodies, and as a result, they have been conducted in accordance with the Helsinki ethical standards and the Social Science guidance. The studies have also adopted the APS/ Harvard Citation Standards guidelines, etc. The authors abide by the publication regulations,
4. Disclaimer: Professional education, awareness, and public welfare and care are not meant to be replaced by this study paper or the information on another website; rather, they are supplied solely for educational purposes. Since everyone has different needs depending on their psychological state, readers should confirm whether the information applies to their circumstances by consulting their wards, teachers, and subject matter experts.
5. Funding: According to the author(s), this article's work is not supported in any way.
6. Data Availability Statement: In accordance with the articles' related data sharing policy, the data supporting the findings of this study will be available upon request. Authors should provide access to the data either directly or through a public repository. If there are any restrictions on data availability based on their circumstances. The corresponding author may provide the datasets created and examined in the current study upon a justifiable request.
Generating HTML Viewer...
− Conflict of Interest
The authors declare no conflict of interest.
− Ethical Approval
Not applicable
− Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].