



IntelliPaper
Abstract
Artery of Percheron (AOP) infarcts are rare ischemic strokes resulting from occlusion of a solitary arterial variant supplying the paramedian thalami and rostral midbrain. We present the case of a 26-year-old previously healthy female who presented with acute altered consciousness and vertical gaze palsy. MRI brain revealed symmetric bilateral thalamic diffusion restriction, consistent with AOP infarction. This case underscores the importance of considering this rare stroke subtype in young patients presenting with unexplained coma or altered mental status.
Explore Digital Article Text
I. INTRODUCTION
The Artery of Percheron (AOP) is an uncommon vascular variant in which a single perforating branch from one posterior cerebral artery supplies both paramedian thalami and occasionally the rostral midbrain. An occlusion in this artery typically leads to bilateral thalamic infarction, sometimes extending to the midbrain, and presents with a variety of neurological signs, most notably impaired consciousness, vertical gaze palsy, and memory disturbances (Lazzaro et al., 2010).
Because of its rarity and the subtle findings on initial imaging, AOP infarction may be underdiagnosed, particularly in young individuals who lack traditional stroke risk factors. Prompt recognition is crucial for proper management and to mitigate potential long-term neurological deficits (Arauz et al., 2014).
II. CASE PRESENTATION
A 26-year-old previously well female was found unresponsive at home by family members. She had complained of a mild headache the night before but had no history of trauma, infection, or substance use. There was no preceding seizure activity or fever. Her medical, drug, and family history were unremarkable.
Glasgow Coma Scale (GCS): 7 (E2V2M3)
Vital signs: Within normal limits.
Neurological Examination: Decreased responsiveness, vertical gaze palsy, preserved pupillary reflexes, and mild right-sided hemiparesis. Plantar responses were flexor bilaterally. No neck stiffness or photophobia.
Initial labs: Normal full blood count, electrolytes, renal and liver function, coagulation profile; negative urine drug screen
Imaging
CT Brain (non-contrast): No acute hemorrhage or early ischemic changes.
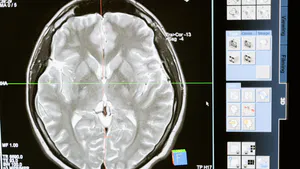
MRI Brain with DWI: Symmetric diffusion restriction in bilateral paramedian thalami, consistent with AOP infarction.
MRA/CTA: Normal Circle of Willis anatomy except for non-visualization of the AOP (as expected); no evidence of vertebrobasilar stenosis
Further Workup
Echocardiogram (TTE + bubble study): Demonstrated a patent foramen ovale (PFO) with right-to-left shunt.
Holter Monitoring (72h): Sinus rhythm Thrombophilia screen: Negative
Infectious and Autoimmune panels: Unremarkable
• Lumbar puncture- Unremarkable
Management
The patient was admitted to the stroke unit and received supportive care. Antiplatelet therapy (aspirin 300 mg) was initiated. No thrombolysis was given due to late presentation beyond the therapeutic window.
Given the presence of a patent foramen ovale (PFO), the stroke team initiated discussions with cardiology regarding the appropriateness of PFO closure to reduce the risk of recurrent embolic events.
Rehabilitation was initiated early with physiotherapy, occupational therapy, and speech therapy input. Over the next two weeks, her mental status gradually improved. Vertical gaze palsy persisted, but memory and motor function improved significantly. She regained functional independence over the next few weeks in basic activities of daily living and was discharged to a to acute stroke care unit? facility for ongoing therapy and then subsequently home.
Neuropsychological testing revealed mild anterograde memory impairment but preserved executive function and language skills.
III. DISCUSSION
AOP infarctions are estimated to represent a small fraction of all ischemic strokes and comprise a notable percentage of bilateral thalamic strokes (Lazzaro et al., 2010). They often manifest with a triad of symptoms: altered consciousness, oculomotor disturbances—particularly affecting vertical gaze—and cognitive or memory deficits.
The thalamus plays a vital role in processing sensory and motor signals, as well as regulating consciousness and alertness. Damage to both paramedian thalami disrupts these functions, resulting in the profound neurological symptoms observed (Percheron, 1973).
Diagnosing AOP infarction can be challenging due to the subtlety of early imaging changes. CT scans may appear normal initially, making MRI with diffusion-weighted imaging essential for early and accurate detection. MRA and CTA typically do not visualize the AOP directly due to its small size (Matheus & Castillo, 2003).
The management of AOP infarcts follows the standard approach for ischemic strokes, involving supportive care and antiplatelet therapy. Identifying potential embolic sources, such as cardiac anomalies or thrombophilia, is especially important in young patients. Recovery outcomes are variable, ranging from full resolution to persistent neurological deficits (Arauz et al., 2014).
Although our patient was young and lacked conventional vascular risk factors, the identification of a patent foramen ovale suggested a potential cardioembolic etiology, and closure was being actively considered, the clinical and radiological features were classic for AOP infarction. This reinforces the importance of considering anatomical stroke variants in young adults and maintaining a low threshold for advanced imaging when initial CT findings are inconclusive.
IV. CONCLUSION
AOP infarction should be considered in the differential diagnosis of young patients who present with sudden onset of reduced consciousness and vertical gaze abnormalities. Early use of MRI can help avoid diagnostic delays and enable prompt initiation of appropriate therapy and rehabilitation. Comprehensive workup to exclude cardioembolic or prothrombotic causes remains essential, even in previously healthy individuals.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research

Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.

