



IntelliPaper
Abstract
Diabetic foot is a major chronic complication of diabetes mellitus and represents a leading cause of hospitalisation, infection and non- traumatic lower limb amputation worldwide. The pathogenesis is multifactorial primarily involving peripheral neuropathy, peripheral arterial disease, impaired immunity and poor glycemic control which together predispose patients to ulceration and delayed wound healing. This review of literature aims to summarise current evidence regarding epidemiology, risk factors clinical evaluation and treatment strategies for diabetic foot disease. The literature consistently demonstrates that early identification of at-risk patients through routine screening and structured risk stratification significantly reduces ulcer occurrence. Management of established diabetic foot ulcers requires a multi-disciplinary approach combining glycemic control, infection management using culture guided antimicrobial therapy, regular wound debridement, appropriate wound dressings and appropriate offloading techniques.In patients with associated ischaemia, timely vascular assessment followed by endovascular or surgical revascularisation is critical for limb salvage. Advanced adjunctive therapies including negative pressure wound therapy, bioengineered skin substitutes and growth factor- based treatments have shown beneficial outcomes in selected cases. Overall, comprehensive preventive programs and standardised multidisciplinary treatment protocols remain essential for reducing amputation rates and improving functional outcomes in patients with diabetic foot disease.
Explore Digital Article Text
Introduction
Diabetes remains a major global health challenge, driving significant morbidity, mortality, and economic strain. Among its many complications, diabetic foot also represents one of the most debilitating outcomes, with diabetes and serving as the leading cause of non-traumatic lower limb amputation worldwide.
WHO defines diabetic foot as Infection, ulceration or destruction of deep tissues associated with neurological abnormalities and various degrees of peripheral vascular diseases in the lower limb. Diabetic foot ulcers emerge from a complex interaction of peripheral neuropathy, peripheral arterial disease, and impaired wound healing, usually exacerbated by infection. Beyond localised tissue damage, diabetic foot ulceration reflects widespread systemic vascular disease and increases risk of cardiovascular morbidity and early mortality. Major lower limb amputations carry a grave prognosis with post-amputation five year mortality exceeding 50% in patients with diabetes.
In India, diabetic foot disease represents a particularly significant public health burden, with an estimated 40,000 amputations performed annually. A large proportion of these amputations are neuropathic in origin and complicated by secondary infection, many of which are potentially preventable.
Several factors predict poor outcomes in individuals with diabetic foot ulcer, including severity, prolonged duration, infection, peripheral arterial disease, neuropathy, chronic kidney disease, cardiovascular disease, smoking, and male gender. These variables influence healing rates, recurrence, and likelihood of progression to major amputation or death. In India sociocultural factors such as barefoot walking, low socioeconomic status, illiteracy, delayed healthcare seeking and reliance on alternative systems of medicine further contribute to late presentation and poor outcomes.
Effective management of diabetic foot ulcers and their associated complications requires a comprehensive, evidence-based approach. Core components of treatment include appropriate pressure offloading, prompt and adequate control of infection, timely revascularisation (when indicated), surgical assessment (where necessary), optimisation of glycemic control and systematic management of coexisting medical conditions. Given the multifactorial pathophysiology of diabetic foot disease, improved clinical outcomes are more likely when care is delivered through a coordinated, multidisciplinary team approach involving interprofessional collaboration.
REVIEW OF LITERATURE
Burden of Diabetic Foot Disease
Hyperglycaemia is associated with various complications, both microvascular- including nephropathy, neuropathy, and retinopathy and macrovascular complications such as coronary artery disease, stroke, and peripheral arterial disease. Among these, diabetic foot disease represents one of the most severe and disabling complications. Diabetes is a leading cause of non-traumatic lower-extremity amputations, with non-healing foot ulcers frequently preceding limb loss.The lifetime risk of developing a foot ulcer in individuals with diabetes ranges between 15% and 20% . With 15% of these ulcers progressing to foot or limb amputation . Population-based studies report an annual incidence of diabetic foot ulcers ranging from 0.5% to 3%, while prevalence varies between 2% and 10% . Approximately 45–60% of diabetic foot ulcers are neuropathic, while nearly 45% exhibit combined neuropathic and ischemic components . Infection is implicated in nearly half of lower-limb amputations in diabetic patients .
Risk Factors
Diabetic foot ulcers arise from an interaction of multiple factors. With peripheral neuropathy comes a loss of sensation, which allows repeated trauma to go unnoticed. Motor neuropathy causes muscle imbalance and foot deformities, resulting in abnormal plantar pressure and callus formation, while autonomic neuropathy reduces sweating, causing dry and fissured skin.Arterial insufficiency further complicates neuropathic ulcers by impairing tissue perfusion and delaying wound healing. Mechanical stress at the wound site plays a significant role in ulcer persistence . Additional risk factors include poor glycemic control, long duration of diabetes, trauma, inappropriate footwear, callus formation, history of previous ulceration or amputation, advancingage, visual impairment, chronic kidney diseaseand poor nutritional status. Infections contribute to chronicity by furtherworsening wound healing leading to a non healing ulcer. Interestingly, a deficiency of Vitamin D is an emerging risk factor for diabetic foot infection .
Classification of Wounds
The Red–Yellow–Black wound classification system by Marion Laboratories categorizes wounds based on the following characteristics :
• Necrotic tissue: Black or dark green in colour, which may be dry or infected
• Sloughy tissue: A yellow, glutinous tissue composed of wound exudate and debris, often mistaken for infection.
• Granulating tissue: Red, vascular tissue indicating active healing
• Epithelializing tissue: Pink in colour, indicating epithelium growing over the wound by keratinocyte migration from wound margins
The presence of devitalised tissue or critical colonisation prevents chronic wounds from healing hence, necessitates removal through debridement of tissue. However, debridement may be contraindicated in purely arterial ulcers . With regular excision of necrotic tissue and surrounding callus we are likely to see accelerated wound healing and an increased likelihood of complete secondary closure .
Grading of Diabetic Foot Ulcers
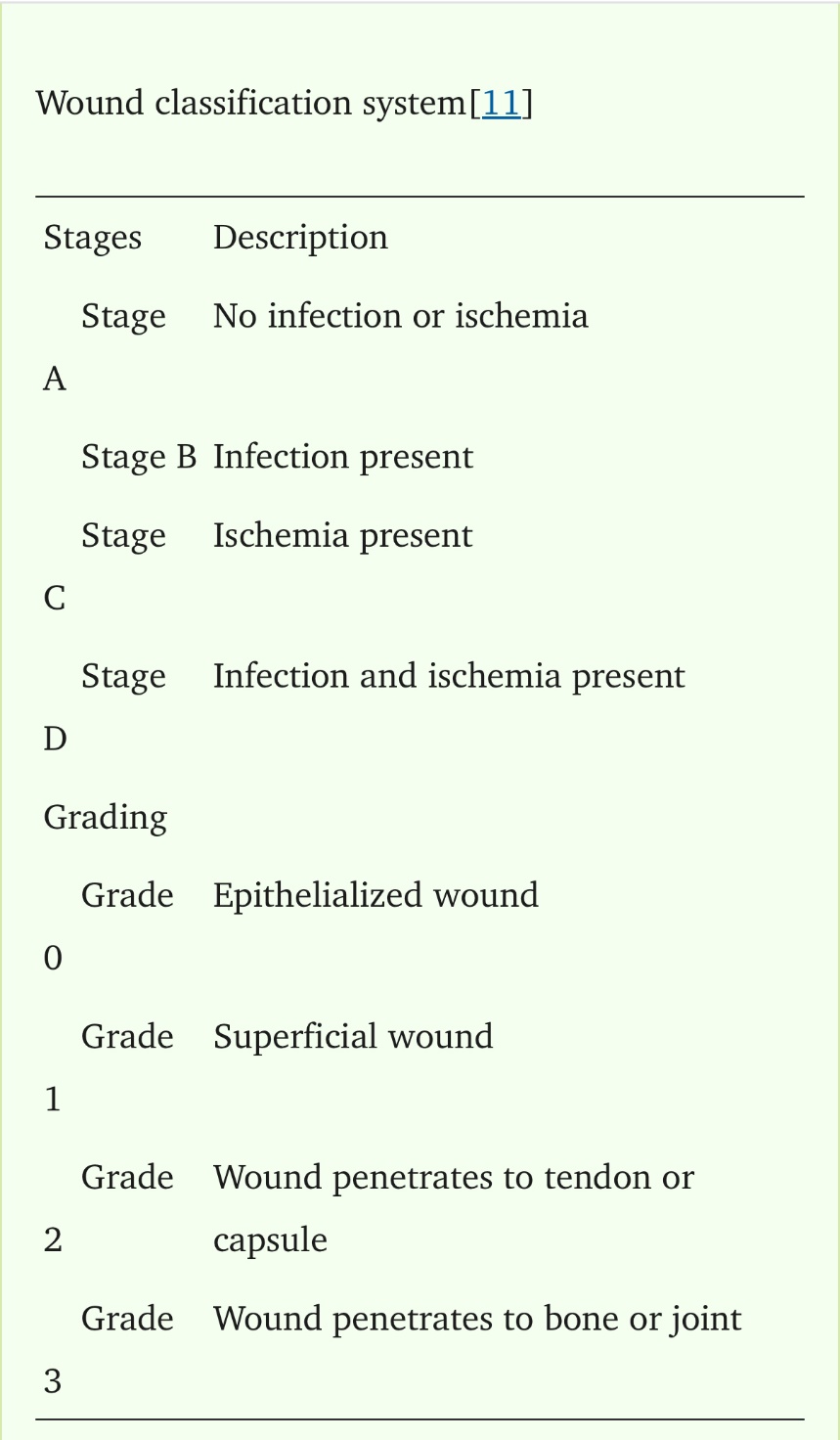
Wound grading is performed using Wagner’s classification or the University of Texas wound classification system . It includes wound depth, infection, and ischemia. To adequately treat am ulcer, a thorough wound assessment is necessary including documentation of the ulcer location, size, depth, wound margins, base, drainage, colour, odour, pain, and progression .
Microbiology of Diabetic Foot Infections
Hyperglycaemia, impaired immune response, neuropathy, and peripheral arterial disease predispose patients to diabetic foot infections .
Diabetic foot infections may involve aerobic, anaerobic, or fungal organisms. With both mono-microbial and poly-microbial infections being quite common . Organisms that most commonly infect diabetic foot ulcers include Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa, with both gram positive and gram negative bacteria showing a similar predominance. Due to theregional variability in microbial patterns, culture-guided antibiotic therapy is required for adequate resolution.
DISCUSSION
Diabetic foot disease remains one of the most feared and debilitating complications of diabetes mellitus. It is associated with prolonged hospitalisations, substantial financial burden, repeated surgical interventions, and a persistent risk of limb loss, all of which significantly affect the physical and psychological well-being of patients. The possibility of amputation and the subsequent experience of phantom limb pain further contribute to emotional distress and reduced quality of life. Consequently, diabetic foot disease continues to pose a major challenge for patients, caregivers, and healthcare systems.
Clinically, the diabetic foot is characterised by a classical triad of neuropathy, ischaemia, and infection with each component contributing to ulcer formation, progression, and poor healing outcomes. These factors rarely act in isolation; instead, their coexistence creates a complex pathological environment that predisposes the foot to breakdown and chronic infection. Preventive strategies therefore are the most effective means of reducing morbidity.
Pathogenesis
The development of diabetic foot ulcers is multifactorial, with peripheral neuropathy and ischemia serving as the primary underlying mechanisms. Continuous weight-bearing and shear forces exacerbate tissue damage, leading to progressive ulceration. Charcot arthropathy represents an advanced manifestation of neuropathy, resulting from a combination of motor, sensory, and autonomic dysfunction, ultimately causing joint instability, altered foot architecture, and increased risk of ulceration.
Peripheral vascular disease further compromises wound healing by reducing tissue perfusion. Although atherosclerosis in diabetic patients resembles that seen in non-diabetics, it tends to be more diffuse, occurs earlier, and progresses more rapidly. In diabetic individuals, distal vessels below the knee are more commonly involved, while pedal arteries may remain relatively spared. The coexistence of ischemia and neuropathy significantly increases the risk of ulceration and limb loss.
Infection and Osteomyelitis
Infection in the diabetic foot is a limb-threatening condition due to the unique anatomical characteristics of the foot, including multiple intercommunicating compartments that facilitate rapid spread. The absence of pain due to neuropathy allows continued ambulation, further propagating infection. Soft tissue structures such as fascia, tendons, and muscle sheaths provide little resistance to infection, and the presence of hyperglycemia and ischaemia impairs host defense mechanisms.
Osteomyelitis commonly develops as a result of contiguous spread from deep soft tissue infections and is frequently associated with chronic or longstanding ulcers. Diagnosis can be challenging and requires careful clinical evaluation, supported by imaging and microbiological studies. Probing to bone remains a useful bedside test, while magnetic resonance imaging offers high sensitivity and specificity for detecting bone involvement. Definitive diagnosis requires bone biopsy for culture and histopathology.
Classification and Assessment
Accurate classification of diabetic foot ulcers is essential for guiding management. Diabetic foot lesions are broadly categorized into neuropathic and neuroischemic types, each requiring distinct therapeutic strategies. The University of Texas Wound Classification System is widely accepted due to its ability to incorporate depth, infection, and ischemia .
Examination of the Feet
Assessment of the feet is a fundamental component of routine physical examination, particularly in individuals with diabetes. Inspection should focus on identifying features suggestive of neuropathy, including xerosis, fissuring, structural deformities, callus formation, altered foot architecture, ulceration, dilated superficial veins, and nail abnormalities. The interdigital spaces must be examined carefully, as lesions in these areas may be easily overlooked. Clinical signs indicative of significant ischemia include loss of hair over the dorsum of the foot and the presence of dependent rubor. Palpation: To assess temperature differences, noting areas of unusual warmth or coolness. Peripheral arterial pulses must be evaluated systematically. The dorsalis pedis artery is palpated lateral to the tendon of extensor hallucis longus, while the posterior tibial artery is felt posterior and inferior to the medial malleolus. Examination should also include palpation and auscultation of the femoral artery to detect bruits. The plantar surface should be assessed for bony prominences, areas of increased pressure, or callosities that may predispose to ulcer formation. Evaluation for sensory neuropathy can be performed using Semmes–Weinstein monofilaments or biothesiometry. In resource-limited settings, simpler bedside methods—such as testing light touch with cotton wool, assessing pinprick sensation, and evaluating vibration perception using a 128 Hz tuning fork—are acceptable alternatives. The primary objective of sensory testing is to determine the presence of loss of protective sensation (LOPS), which significantly increases the risk of ulceration. A handheld Doppler device may be employed to verify arterial flow and further assess vascular status. When combined with a sphygmomanometer, measurement of ankle and brachial systolic pressures allows calculation of the ankle–brachial index (ABI). Under normal circumstances, ankle systolic pressure slightly exceeds brachial pressure, yielding an ABI greater than 1. An ABI value below 0.9, particularly when accompanied by diminished or absent pulses, is indicative of peripheral arterial disease. Conversely, palpable pulses with an ABI above 1 generally exclude significant ischemia .
Revascularization
Individuals presenting with significant peripheral ischaemia need re-establishment of arterial perfusion, as sufficient blood supply is critical for effective wound healing and eradication of infection. In cases of inadequate circulation tissue repair gets compromised the likelihood of limb loss drastically increases. Bypass surgery continues to be a well-recognised intervention for ischemic lower extremities, with durable long-term outcomes reported. Limb salvage rates of nearly 90% at 10 years have been documented following lower extremity bypass procedures . In cases where arterial disease involves multiple segments, revascularization should target each level of obstruction to restore adequate distal blood flow and enhance the probability of limb preservation. Percutaneous transluminal angioplasty is particularly appropriate for discrete, short-segment stenotic lesions. Conversely, when disease is extensive—characterised by multiple occlusions, lesions longer than 15 cm, or infra-popliteal vessel involvement—bypass surgery is generally regarded as the treatment of choice. .
Prevention
Timely identification of individuals at risk for ulceration plays a crucial role in preventing the development of diabetic foot lesions. An effective screening method includes- annual foot examinations for all patients with diabetes to initiate early intervention.Patient education forms the cornerstone of prevention strategies. Individuals should be counselled about strict glycemic control, use of appropriate footwear, avoiding foot trauma and routine self-inspection of the feet.
Preventive strategies may be categorised into three levels:
• Primary prevention: Identification of high-risk feet and provision of guidance regarding protective or therapeutic footwear.
• Secondary prevention: Early management of minor foot problems, including callus care, treatment of nail disorders, and appropriate handling of blisters or superficial lesions.
• Tertiary prevention: Early referral to specialised centers for advanced or complicated foot lesions .
Improved limb salvage rates and reduction in amputation incidence can be achieved through structured training of primary care physicians and paramedical staff in diabetic foot management. The “Step by Step” program, implemented by the World Diabetes Foundation, represents one such initiative .
Continuous patient education and long-term follow-up are essential for all individuals suffering with diabetes, especially diabetic foot ulcers. Such patients should be advised to limit excessive mechanical stress on the affected limb and adopt activity modifications when necessary.A comprehensive understanding of diabetic foot pathology, systematic foot examination, appropriate classification of ulcers, multidisciplinary management, and implementation of preventive measures collectively contribute to improved limb preservation and reduced amputation rates among individuals with diabetes.
Conclusion
Diabetic foot disease remains a major and largely preventable cause of morbidity among individuals with diabetes mellitus and continues to contribute for a significant proportion of hospitalisation and non-traumatic lower-limb amputations worldwide. This literature review consistently demonstrates that diabetic foot complications arise from the interaction of peripheral neuropathy, peripheral arterial disease, infection, foot deformities and poor glycaemic control; additionally delayed presentation and inadequate preventive care further exacerbates disease severity and adversely affect clinical outcomes.
Evidence strongly supports the effectiveness of preventive strategies including routine foot screening, risk stratification, patient education, use of appropriate footwear and early referral to specialised diabetic foot clinics. Multidisciplinary care models involving surgeons, diabetologists, podiatrists, vascular specialists and wound care teams have been shown to significantly reduce ulcer recurrence and amputation rates. In terms of treatment, the literature highlights that successful management requires a structured stepwise approach consisting of optimal glycaemic control, aggressive infection management using culture-guided antimicrobial therapy, regular wound debridement, appropriate wound dressings and effective off-loading techniques such as total contact casting or customised orthotic devices. In patients with ischaemic limbs, timely vascular assessment and revascularisation procedures, either endovascular or surgical, play a crucial role in improving limb salvage. Advanced wound-care modalities, including negative pressure wound therapy, growth factor-based therapies, and skin substitutes have demonstrated promising adjunctive benefits in selected cases. In summary, diabetic foot disease is largely preventable and treatable when addressed through early detection, standardised treatment protocols and coordinated multidisciplinary care. Strengthening preventive services, ensuring timely surgical and vascular interventions and expanding access to comprehensive diabetic foot management programs remain essential steps in reducing the burden of amputations and improving long-term patient outcomes.
-
Kavitha KV. Choice of wound care in diabetic foot ulcer: A practical approach. World Journal of Diabetes . 2014;5(4):546–56. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4127589/
-
Boulton AJM, Whitehouse RW. The Diabetic Foot . Share.google. MDText.com, Inc.; 2023 . Available from: https://share.google/lmihDDsq4EWv5x33P
-
Pendsey S. Understanding diabetic foot. International Journal of Diabetes in Developing Countries . 2010;30(2):75. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2878694/
-
Barnes LA, Marshall CD, Leavitt T, Hu MS, Moore AL, Gonzalez JG, et al. Mechanical Forces in Cutaneous Wound Healing: Emerging Therapies to Minimize Scar Formation. Advances in Wound Care. 2018 Feb;7(2):47–56.
-
Danny Darlington CJ, Suresh Kumar S, Jagdish S, Sridhar MG. Evaluation of Serum Vitamin D Levels in Diabetic Foot Infections: A Cross-Sectional Study in a Tertiary Care Center in South India. Iranian Journal of Medical Sciences . 2019 Nov 1 ;44(6):474–82. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6885722/
-
Labib A, Winters R. Complex Wound Management . Nih.gov. StatPearls Publishing; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK576385/
-
Dawi J, Tumanyan K, Tomas K, Misakyan Y, Gargaloyan A, Gonzalez E, et al. Diabetic Foot Ulcers: Pathophysiology, Immune Dysregulation, and Emerging Therapeutic Strategies. Biomedicines. 2025 Apr 29;13(5):1076.
-
Shi Y, Li H, Yuan B, Wang X. Effects of multidisciplinary teamwork in non-hospital settings on healthcare and patients with chronic conditions: a systematic review and meta-analysis. BMC Primary Care . 2025 Apr 15;26(1). Available from: https://bmcprimcare.biomedcentral.com/articles/10.1186/s12875-025-02814-0
-
Ozgok Kangal MK, Regan JP. Wound Healing . Nih.gov. StatPearls Publishing; 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535406/
-
IDF Diabetes. Chapter 2: The global burden. 2013. pp. 29–49. Available from: http://www.idf.org/sites/default/ files/EN_6E_Ch2_the_Global_Burden.pdf.
-
Manna B, Morrison CA, Nahirniak P. Wound Debridement . National Library of Medicine. StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507882/
-
3. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293:217–228. doi: 10.1001/jama.293.2.217.
-
3.Reiber GE. Epidemiology and health care costs of diabetic foot problems. In: Veves A, Giurini JM, LoGerfo FW, editor(s) , editors. The Diabetic Foot. New Jersey: Humana Press; 2002. pp. 35–58.
-
Frykberg RG, Zgonis T, Armstrong DG, Driver VR, Giurini JM, Kravitz SR, Landsman AS, Lavery LA, Moore JC, Schuberth JM, et al. Diabetic foot disorders. A clinical practice guideline (2006 revision) J Foot Ankle Surg. 2006;45:S1–66. doi: 10.1016/S1067-2516(07)60001-5.
-
Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery LA, Boulton AJ. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care. 1999;22:157–162. doi: 10.2337/diacare.22.1.157.
-
Richard JL, Sotto A, Lavigne JP. New insights in diabetic foot infection. World J Diabetes. 2011;2:24–32. doi: 10.4239/wjd.v2.i2.24.
-
Farahani RM, Kloth LC. The hypothesis of ‘biophysical matrix contraction’: wound contraction revisited. Int Wound J. 2008;5:477–482. doi: 10.1111/j.1742-481X.2007.00402.x.
-
Kranke P, Bennett MH, Martyn-St James M, Schnabel A, Debus SE, Weibel S. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database of Systematic Reviews. 2015 Jun 24;
-
Carolina W, Geoff S. Wound dressings update. J Pharm Pract Res. 2006;36:318–324.
-
Falanga V. Wound healing and its impairment in the diabetic foot. Lancet. 2005;366:1736–1743. doi: 10.1016/S0140-6736(05)67700-8.
-
Falanga V. Wound bed preparation: science applied to practice. In: European wound management association (EWMA), editor. Position Document. Wound Bed Preparation in Practice. London: MEP Ltd; 2004. pp. 2–5. Available from: http://www.ewma.org/
-
Miller M. The role of debridement in wound healing. Community Nurse. 1996;2:52–55.
-
Steed DL, Donohoe D, Webster MW, Lindsley L. Effect of extensive debridement and treatment on the healing of diabetic foot ulcers. Diabetic Ulcer Study Group. J Am Coll Surg. 1996;183:61–64.
-
Steed D. Modulating wound healing in diabetes. In: Levin and O’Neal’s., editor. The Diabetic Foot. St Louis: J Bowker and M Pfeiffer; 2001. pp. 395–404.
-
Armstrong DG, Lavery LA, Harkless LB. Validation of a diabetic wound classification system. The contribution of depth, infection, and ischemia to risk of amputation. Diabetes Care. 1998;21:855–859. doi: 10.2337/diacare.21.5.855.
-
Enoch S, Grey JE, Harding KG. ABC of wound healing. Non-surgical and drug treatments. BMJ. 2006;332:900–903. doi: 10.1136/bmj.332.7546.900.
-
Lipsky BA. A report from the international consensus on diagnosing and treating the infected diabetic foot. Diabetes Metab Res Rev. 2008;20 Suppl 1:S68–S77. doi: 10.1002/dmrr.453.
-
Calhoun JH, Cantrell J, Cobos J, Lacy J, Valdez RR, Hokanson J, Mader JT. Treatment of diabetic foot infections: Wagner classification, therapy, and outcome. Foot Ankle. 1988;9:101–106. doi: 10.1177/107110078800900301.
-
Wu L, Norman G, Dumville JC, O’Meara S, Bell-Syer SE. Dressings for treating foot ulcers in people with diabetes: an overview of systematic reviews. Cochrane Database of Systematic Reviews. 2015 Jul 14;(7).
-
Vishwanathan V, Thomas N, Tandon N, Asirvatham A, Rajasekar S, Ramachandran A, Senthilvasan K, Murugan VS, Muthulakshmi Profile of diabetic foot complications and its associated complications - a multicentric study from India. J Assoc Physicians India. 2005;53:933–936.
-
Lavery LA, Armstrong DG, Wunderlich RP, Tredwell J, Boulton AJ. Predictive value of foot pressure assessment as part of a population-based diabetes disease management program. Diabetes Care. 2003;26:1069–1073. doi: 10.2337/diacare.26.4.1069.
-
Gadepalli R, Dhawan B, Sreenivas V, Kapil A, Ammini AC, Chaudhry R. A clinico-microbiological study of diabetic foot ulcers in an Indian tertiary care hospital. Diabetes Care. 2006;29:1727–1732. doi: 10.2337/dc06-0116.
-
Citron DM, Goldstein EJ, Merriam CV, Lipsky BA, Abramson MA. Bacteriology of moderate-to-severe diabetic foot infections and in vitro activity of antimicrobial agents. J Clin Microbiol. 2007;45:2819–2828. doi: 10.1128/JCM.00551-07.
-
Ramakant P, Verma AK, Misra R, Prasad KN, Chand G, Mishra A, Agarwal G, Agarwal A, Mishra SK. Changing microbiological profile of pathogenic bacteria in diabetic foot infections: time for a rethink on which empirical therapy to choose? Diabetologia. 2011;54:58–64. doi: 10.1007/s00125-010-1893-7.
-
Abdulrazak A, Bitar ZI, Al-Shamali AA, Mobasher LA. Bacteriological study of diabetic foot infections. J Diabetes Complications. 2005;19:138–141. doi: 10.1016/j.jdiacomp.2004.06.001.
-
Raja NS. Microbiology of diabetic foot infections in a teaching hospital in Malaysia: a retrospective study of 194 cases. J Microbiol Immunol Infect. 2007;40:39–44.
-
Bansal E, Garg A, Bhatia S, Attri AK, Chander J. Spectrum of microbial flora in diabetic foot ulcers. Indian J Pathol Microbiol. 2008;51:204–208. doi: 10.4103/0377-4929.41685.
-
Singh SK, Gupta K, Tiwari S, Shahi SK, Kumar S, Kumar A, Gupta SK. Detecting aerobic bacterial diversity in patients with diabetic foot wounds using ERIC-PCR: a preliminary communication. Int J Low Extrem Wounds. 2009;8:203–208. doi: 10.1177/1534734609353080.
-
Tiwari S, Pratyush DD, Dwivedi A, Gupta SK, Rai M, Singh SK. Microbiological and clinical characteristics of diabetic foot infections in northern India. J Infect Dev Ctries. 2012;6:329–332. doi: 10.3855/jidc.1827.
-
Vijaykumar H. Comparative study of collagenase and papain-urea based preparations in the management of chronic nonhealing limb ulcers. Indian Journal of Science and Technology. 2011 Sep 20;4(9):1090–100.
-
Huang C, Wang R, Yan Z. Silver dressing in the treatment of diabetic foot. Medicine. 2021 Feb 19;100(7):e24876.
-
Junker JPE, Kamel RA, Caterson EJ, Eriksson E. Clinical Impact Upon Wound Healing and Inflammation in Moist, Wet, and Dry Environments. Advances in Wound Care. 2013;2(7):348–56.
-
Shanmugam P, M J, Susan S L. The bacteriology of diabetic foot ulcers, with a special reference to multidrug resistant strains. J Clin Diagn Res. 2013;7:441–445. doi: 10.7860/JCDR/2013/5091.2794.
-
Aderibigbe BA, Buyana B. Alginate in Wound Dressings. Pharmaceutics . 2018 Apr 2;10(2):42. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6027439/
-
Boulton AJ. Pressure and the diabetic foot: clinical science and offloading techniques. Am J Surg. 2004;187:17S–24S. doi: 10.1016/S0002-9610(03)00297-6.
-
Consensus development conference on diabetic foot wound care. 7-8 April 1999, Boston, MA. American Diabetes Association. Adv Wound Care. 1999;12:353–361.
-
Sumpio BE, Aruny J, Blume PA. The multidisciplinary approach to limb salvage. Acta Chir Belg. 2004;104:647–653. doi: 10.1080/00015458.2004.11679637.
-
Bennett NT, Schultz GS. Growth factors and wound healing: biochemical properties of growth factors and their receptors. Am J Surg. 1993;165:728–737. doi: 10.1016/s0002-9610(05)80797-4.
-
Basile P, Rosenbloom B. Local care of the diabetic foot. In: Veves A, Giurini JM, LoGerfo FW, editor(s) , editors. The Diabetic Foot. New Jersey: Humana Press; 2002. pp. 279–292.
-
Sibbald RG, Williamson D, Orsted HL, Campbell K, Keast D, Krasner D, Sibbald D. Preparing the wound bed--debridement, bacterial balance, and moisture balance. Ostomy Wound Manage. 2000;46:14–22, 24-8, 30-35; quiz 36-37.
-
R, editor. St. Louis: Mosby; 2000. pp. 85–124.
-
Ramundo J, Gray M. Enzymatic wound debridement. J Wound Ostomy Continence Nurs. 2008;35:273–280. doi: 10.1097/01.WON.0000319125.21854.78.
-
Sherman RA, Wyle F, Vulpe M. Maggot therapy for treating pressure ulcers in spinal cord injury patients. J Spinal Cord Med. 1995;18:71–74. doi: 10.1080/10790268.1995.11719382.
-
Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB. Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care. 2001;24:1019–1022. doi: 10.2337/diacare.24.6.1019.
-
Brem H, Sheehan P, Boulton AJ. Protocol for treatment of diabetic foot ulcers. Am J Surg. 2004;187:1S–10S. doi: 10.1016/S0002-9610(03)00299-X.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research




Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.
