




IntelliPaper
Abstract
Every second patient who dies from congenital heart disease is an infant with heart failure. However, infants were de facto excluded from the US Carvedilol trial and PANORAMA HF trial (Sacubitril/Valsartan), probably due to their high mortality risk. Despite the negative results of the US Enalapril trial in infants with univentricular hearts, ACE inhibitors are further recommended in the guidelines. Propranolol is the only drug that has been successful in two prospective randomized trials but was not recommended in the guidelines.
This review discusses the dif erences between myocardial heart failure and congestive circulatory failure in infants with congenital heart disease that do not benefit from vasodilators but from beta-blockers that significantly improve clinical symptoms, neurohormonal activation and heart rate variability.
The case of a non-invasive monitoring of heart rate variability, blood pressure and oxygen saturation of an infant with Down syndrome and complete atrioventricular septal defect visualize cardiac decompensation after enalapril and the benefits of beta-blocker treatment.
Explore Digital Article Text
THE HISTORY OF HEART FAILURE IN INFANTS WITH CONGENITAL HEART DISEASE
Heart failure in infants with congenital heart disease — the most common birth defect — is closely related to prognosis. Every second patient who died from congenital heart disease is an infant. Retrospective data from Germany show the improvement in the prognosis of patients with congenital heart disease due to successful heart surgery. However, heart failure in infancy remains the most frequent cause of death (Table 1), as currently confirmed by Swedish register data. Despite approximately 4000 additional percutaneous interventions yearly in Germany, the mortality from congenital heart defects has actually been rising again since 2010. The hypothesis of a link of this rising mortality and an irrational heart failure therapy in infants with congenital heart defects will be explained.
| 1931–1963 (N=275) | 1963–1966 (N=163) | 2005 (N=1755) | |
|---|---|---|---|
| Mortality | 44% (121) | 31% (108) | 6.3% (111) |
| Death from Heart Failure | 82% (99) | 66% (71) | 74% (82) |
| Death in Infancy | 92% (111) | 88% (143) | 67% (74) |
Retrospective Single Center Data of Children with Congenital Heart Disease from Germany
THE PATHOPHYSIOLOGY OF HEART FAILURE IN INFANTS WITH CONGENITAL HEART DISEASE
Pharmacotherapy of heart failure depends on evolving pathophysiological models, which are predominantly developed on left ventricular dysfunction in adults. The neurohormonal hypothesis of Milton Packer led to an improvement in the prognosis of adults with reduced ejection fraction (HFrEF), as shown in a lot of prospective, randomized trials.
More than 65 years ago, Katz, Feinberg and Shaffer were the first who make a distinction of heart failure either as “myocardial failure” (today HFrEF) or “congestive circulatory failure” as inadequate output associated with volumetric overloading of the systemic or the pulmonary circuits — the predominant cause of heart failure in infants with congenital heart defects.
Unfortunately, the current guidelines for pediatric heart failure as well as the few prospective randomized trials in children with congenital heart disease do not make a clear distinction between “myocardial failure” and “congestive circulatory failure”. Moreover, these trials de facto exclude infants with heart failure due to congenital heart defects. This exclusion of the most vulnerable group of infants with congenital heart disease probably depends on the high mortality in the enalapril trial of infants with univentricular hearts.
The most critical point is the use of vasodilators — designed for adult myocardial failure — in infants with “congestive circulatory failure”. In a review of 350 cases of infants with heart failure due to congenital heart disease, Elton Goldblatt wrote in 1962: “…there is peripheral vasodilatation which normally results in increased cardiac output and venous return. The failing heart cannot adapt to these extra demands; thus, the clinical condition is made worse.” Genetic data now clearly confirm the advantage of blood pressure increasing alleles on outcome in children with congenital heart disease. It must be feared that the misuse of vasodilators as well as ACE inhibitors in infants with heart failure due to congenital heart disease is one of the reasons for the persistently high mortality rate.
Before introducing beta-blocker treatment in infants with severe heart failure due to congenital heart disease in 1996, we carried out extensive measurements of invasive hemodynamics, ventricular function, neurohormonal activation and early life stress. Early life stress was measured by norepinephrine plasma levels and heart rate variability as shown in Figure [fig:impact-dysautonomia]. Arterial hypotension is the most significant hemodynamic cause of tachypnea and neurohormonal activation in these infants. In addition, 24-hours mean heart rate (and heart rate variability) is the most important predictor of tachypnea in infants with heart failure. Recent data now confirm that heart rate variability is an important predictor of prognosis in children with congenital heart disease.
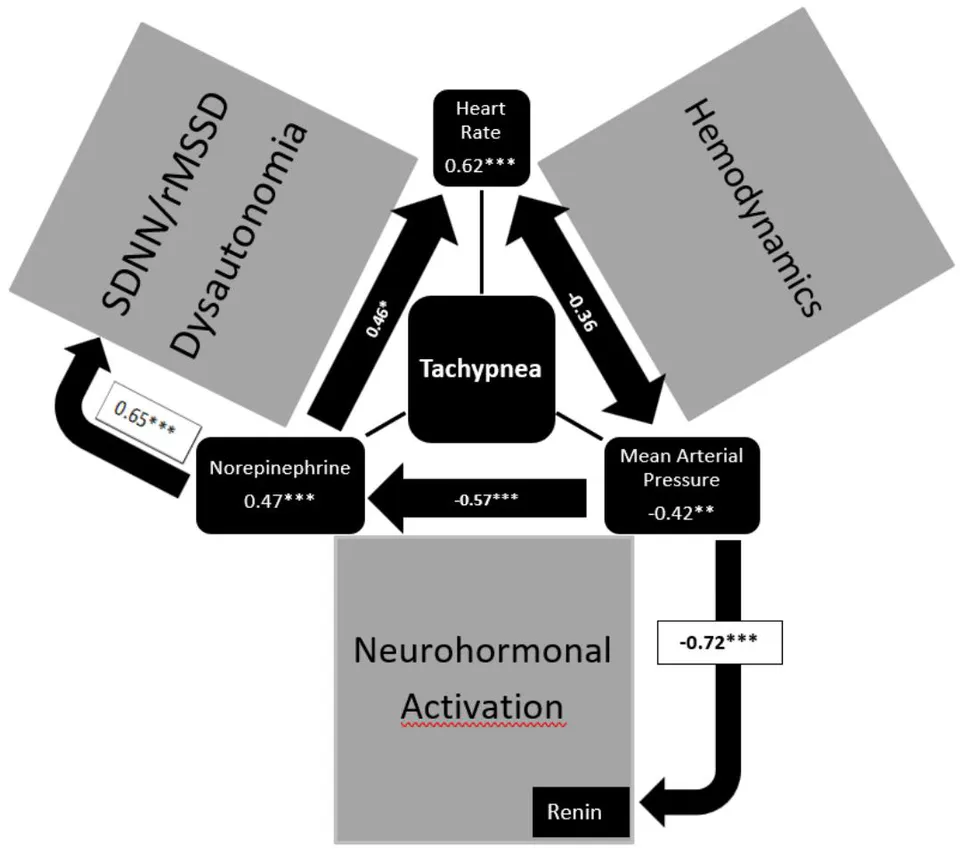
The Impact of Dysautonomia, Hemodynamics and Neurohormonal Activation on Clinical Heart Failure Indicated by the Parameter Tachypnea.
Tachypnea is significantly related to heart rate (), norepinephrine plasma levels () and mean arterial pressure (). The mean arterial pressure has a highly significant impact on plasma renin activity () and norepinephrine levels (). Dysautonomia measured as 24-hour heart rate variability (SDNN/rMSSD) is related to plasma norepinephrine levels ().
PHARMACOTHERAPY OF HEART FAILURE IN INFANTS WITH CONGENITAL HEART DISEASE
The following therapy of heart failure in infants with congenital heart disease was introduced in the 1950s: Digoxin, Sedation, and Diuretics. Today, enalapril seems to be the only “new” innovation as recommended in the current guideline from 2025 (Table 2). However, a prospective randomized trial showed significantly poorer head growth in infants with heart failure treated with enalapril compared to placebo but no improvement of clinical symptoms, weight gain, and prognosis.
The beta-blocker propranolol is the only pharmacotherapy that improves clinical symptoms in two prospective randomized trials in infants with heart failure due to congenital heart disease but was not mentioned in the current guideline. The CHF-Pro-Infant trial clearly shows a significant clinical improvement measured by the Ross Score, lower plasma renin activities and a significant improvement of heart rate variability (Figure [tab:impact-pharmacotherapy]). However, Beta-blockers are traditionally considered contraindicated in pediatric cardiology based on the cardiocirculatory, hemodynamic heart failure model. Unfortunately, this view has not clearly changed even after the convincing prospective beta-blocker trials in adults with heart failure.
With respect to these data (Figure [tab:impact-pharmacotherapy]), pediatric cardiologists are standing at a therapeutic crossroad either to follow the guideline recommendations with Diuretics, ACE inhibitors and vasodilators, that clearly further escalate neurohormonal activation and early life stress or to use beta-blockers, that are not recommended in the guidelines. The current guideline recommendations further prefer pharmacotherapies, which are based upon the cardio-circulatory/hemodynamic heart failure model (Table 2). In infants with circulatory failure, hypotension due to enalapril leads to a counter-regulatory increase of plasma renin activity by 450% as shown in the prospective European LENA project. These data clearly show that an effective inhibition of the renin-angiotensin-aldosterone system is not achieved with enalapril in infants with congenital heart disease. We exclude ACE inhibitors in our trials, after showing this aldosterone escape phenomenon in a retrospective analysis in 2000.
| Escalation | De-escalation | |||
|---|---|---|---|---|
| 3-3 (lr)4-5 Parameter | Pharmacotherapy | Diuretics | ACE Inhibitor | Beta-blocker |
| Prospective Trials | Ross Score | −20%* | −60%** | |
| Norepinephrine | ||||
| Plasma Renin Activity | +406%** | +450%* | −52%* * * | |
| Aldosterone | −59%* | |||
| NT-BNP | ||||
| Heart Rate Variability | Heart rate | −15%** | ||
| SDNN | +47%** | |||
| rMSSD | +79%** | |||
| Model | Therapy | Trial | Year | Guideline 2025 | Note on Infant Use |
|---|---|---|---|---|---|
| Cardio-renal | Diuretics | 350 infants | 1962 | Class I | Retrospective |
| SGLT2 Inhibitors | No infants | May be considered | |||
| Cardio-circulatory/ hemodynamic | Digoxin | 816 infants | 2016 | May be considered | Retrospective interstage mortality |
| Levosimendan | 120 infants | 2026 | Bridge to transplant | Retrospective | |
| Milrinone | infants | 2015 | Palliative setting | Meta-analysis Cochrane | |
| Neurohormonal | Enalapril | 115 infants | 2010 | May be considered | Poorer head growth |
| Sacubitril/ Valsartan | 6 infants | 2025 | Class IIa | Panorama HF Trial | |
| Carvedilol | 1 infant | 2007 | Worsen, caution | US-Carvedilol Trial | |
| -selective BB | 51 infants | 2021 | Bisoprolol HLHS Giessen | ||
| Propranolol | 50 infants | 2001/2013 | Not mentioned | CHF-Pro-Infant, VSD-PHF | |
| Heart rate | Ivabradine | No infants | Is reasonable | Anti-arrhythmic use |
Pharmacotherapy of Heart Failure in Infants with Congenital Heart Disease
CHD: congenital heart disease. Green (implied): benefit in a clinical trial or guideline recommendation. Yellow (implied): no benefit in a clinical trial. Red (implied): disadvantage in a clinical trial or guideline warning.
ECONOMIC AND ETHICAL CONTEXT OF THE DEVELOPMENT OF BETA BLOCKER THERAPY IN INFANTS WITH HEART FAILURE DUE TO CONGENITAL HEART DISEASE
After safety and efficacy of propranolol in infants with severe heart failure due to congenital heart disease has been shown in a prospective randomized trial, beta-blocker therapy in infants heart failure was only investigated at the university Giessen and the All-India Institute of Medical Sciences in the last 25 years. This lack of interest is surprising when one considers that death from heart failure is the second most common cause of infant mortality and the most frequent cause of death in patients with congenital heart disease ( infant deaths/year in Germany). One reason for this lack of interest is that the objective mortality rates of congenital heart defects are very badly communicated up to 2010. The publications of the Pediatric Heart Network’s single Ventricle Reconstruction Trial and Swedish registry data revealed the persistently high mortality, especially in univentricular hearts. At a mean age of 11 years 41% of the original 549 infants of the Pediatric Heart Network’s single Ventricle Reconstruction Trial are dead or transplanted in 2025. The current German data published in 2024 confirm this high mortality.
Research into pediatric heart failure at the University Göttingen was stopped after the decision-makers are convinced that the mortality in infants with congenital heart disease will be improved by the new percutaneous cardiac interventions. Moreover, interventional cardiology promised profits in a rapidly growing market (3796 procedures in 2023). The pharmaceutical industry was not interested in Propranolol therapy for infant heart failure, as no profits were expected.
In this economic and ethical context, beta-blocker therapy of infants with severe heart failure due to congenital heart defects was further developed at a small children’s hospital with low case numbers at the Caritas Hospital in Bad Mergentheim, Germany. In summary, we treated 43 infants with severe heart failure due to congenital heart disease (Ross Score ) from 1996–2020. As shown in Table 3, more than 50% of these very ill infants had chromosome anomalies and all infants suffer from pulmonary hypertension. The 4 infants with univentricular hearts and Down syndrome died. All other infants survive heart surgery without heart failure in later life with perfect neurodevelopment and physical performance.
| Patients (N=43) | AVSD (N=21) | Biv. Repair (N=7) | Univ. Heart (N=12) | Spont. Closure (N=3) | Down Syndrome (N=15) |
|---|---|---|---|---|---|
| Göttingen (N=16) 1996–2004 | 8 | 1 | 7 | 0 | 5 |
| Bad Mergentheim (N=27) 2005–2020 | 13 | 6 | 5 | 3 | 10 |
| Chromosome Anomaly (N=22) | 15 (71%) | 3 (43%) | 4 | 0 | 15 |
| Pulmonary Hypertension | 100% | 100% | 100% | 100% | 100% |
| Mortality (N=4) | 0 | 0 | 4 (33%) | 0 | 4 (27%) |
Our Whole Group of Patients Treated with Propranolol for Severe Heart Failure Due to Congenital Heart Disease (Ross Score ) in Infancy
IMPROVING PHARMACOTHERAPY OF HEART FAILURE IN INFANTS WITH CONGENITAL HEART DISEASE BY NONINVASIVE MONITORING OF HEMODYNAMICS AND HEART RATE VARIABILITY
The question remains, how to treat infants with severe heart failure due to congenital heart disease with a high mortality risk. The guidelines recommend enalapril, who failed to improve clinical symptoms and prognosis in a prospective randomized trial and not take into account propranolol, who improves clinical symptoms, heart rate variability and neurohormonal activation in 2 prospective randomized trials?
In the last 30 years, we only treated the most vulnerable infants with a Ross Score and pulmonary hypertension in a compassionate use setting (Table 3). To ensure the safety of the babies, we monitored them up to 2020 by Holter ECG or HRV-online monitoring on our intensive care unit. Today, we use a non-invasive real-life monitoring of hemodynamics, oxygen saturation and heart rate variability in an outpatient setting as recently published. For therapy control we are aiming the following targets: heart rate (110–130 bpm) and vagus activity measured as High Frequency Power ( ms) or rMSSD ( ms). The available high frequency power data of 24 hours heart rate variability analysis in infants with heart failure are illustrated in Figure [fig:24h-vagus]. We include 6 infants treated from the university hospitals, who prefer the beta blocker metoprolol. The targets were reached in all surviving infants treated with propranolol digoxin. Despite a clinical improvement, the targets are not reached with metoprolol therapy (heart rate bpm, rMSSD ms and high frequency power ms).
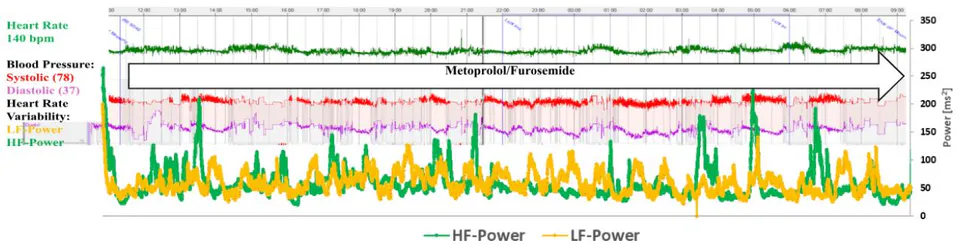
Recently, we had the opportunity to monitor cardiac decompensation of an infant with Down syndrome and complete atrioventricular septal defect during treatment with enalapril, spironolactone and hydrochlorothiazide (Figure [fig:decompensation-enalapril]). The most impressive result is the complete loss of vagus activity measured as high frequency power with a mean heart rate of 150 bpm. The rescue therapy with the inodilator milrinone leads to severe arterial hypotension — measured invasively and noninvasively — that have to be treated with the vasoconstrictor norepinephrine. After introduction of the beta-blocker metoprolol, the vagus activity recovered on a low level with mean heart rate of 140 bpm (Figure [fig:recompensation-metoprolol]) and the baby is gaining weight for the first time in his life.
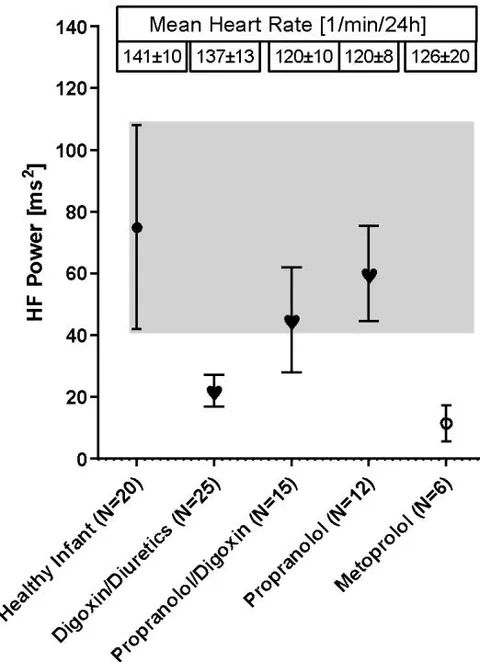
24-Hour Mean Vagus Activities, Measured with Fast Fourier Analysis (HF-Power) and Mean Heart Rates in Infants with Severe Heart Failure Due to Congenital Heart Defects
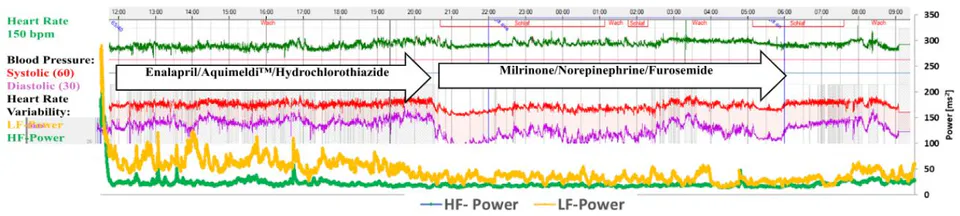
Noninvasive Monitoring of Hemodynamics and Heart Rate Variability after Cardiac Decompensation in an Infant with Atrioventricular Septal Defect Treated with Enalapril
AUTONOMIC IMPRINTING BY EARLY LIFE STRESS: THE DETRIMENTAL CONSEQUENCE OF HEART FAILURE IN INFANTS WITH CONGENITAL HEART DEFECTS ON LONG-TERM PROGNOSIS
Early life stress in infants, measured by norepinephrine plasma levels and heart rate variability, has longtime consequences on growth and neurodevelopment. Congenital heart disease and genetic syndromes showed the largest reductions of heart rate variability in long-term follow up. We introduce the term “autonomic imprinting” to explain the long-term effects of early life stress on the autonomic nervous system. We analyzed somatic growth and heart rate variability up to the 13th year of life of 17 children who are treated with propranolol for heart failure in infancy in Bad Mergentheim. The data show normal vagus activities measured as rMSSD in these children (Table [tab:vagus-activities]) in contrast to older patients after surgery of congenital heart defects who are treated with standard heart failure therapy. We further found a better catch-up growth of length and head circumference (Figure [fig:head-circumference]) compared to a German cohort of children with congenital heart defects. Neonatal head circumference is one of the top 10 candidate variables for longtime neurodevelopmental outcome. Head circumference growth is significantly worse in enalapril treated infants compared to placebo but nearly normal after propranolol treatment of infants with heart failure due to congenital heart defects (Figure [fig:head-circumference]).
| Group | N | Age [Years] | RMSSD [ms/24h] | RMSSD [ms/day] | RMSSD [ms/night] | RMSSD ratio [%] |
|---|---|---|---|---|---|---|
| Grown Up with CHD | 43 | 34.3 12.0 | 47.0 | 39.0 | 53.1 | 146.3 |
| Standard Therapy | 124 | 33.7 10.5 | 39.3 | 35.9 | 43.5 | 117.4 |
| Children | ||||||
| Controls | 59 | 9.8 2.0 | 53.0 17 | 39.2 14.8 | 69.5 24.3 | 186 60 |
| Propranolol Therapy | 17 | 9.6 3.6 | 51.2 35.6 | 34.9 13 | 54.0 19.6 | 160 65 |
Long-term Data of Vagus Activities Measured by Heart Rate Variability (rMSSD) in Patients after Surgery of Congenital Heart Disease, Treated with Beta-Blocker or Standard Therapy in Infancy
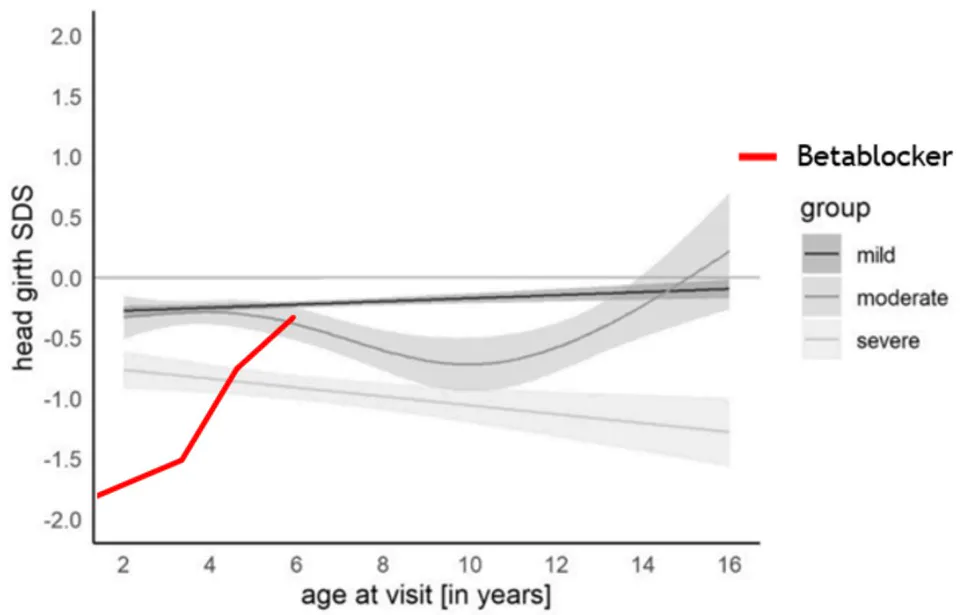
Standard Deviation of the Head Circumferences (SDS) of 14 Patients with Severe Heart Failure Treated with Propranolol in Infancy Compared to the German Average of Children with Congenital Heart Disease Treated with Standard Therapy as Recently Published
CONCLUSION
Despite a very high mortality of infants with severe heart failure due to congenital heart defects, pediatric cardiologists are further standing at a therapeutic crossroad either to follow the guideline recommendations with Diuretics, ACE inhibitors and vasodilators which clearly escalate neurohormonal activation and early life stress or to de-escalate early life stress with beta-blockers, that are not recommended in the guidelines. Propranolol showed a significant benefit of clinical symptoms, neurohormonal activation and heart rate variability in two prospective randomized trials. Enalapril is further recommended in the guidelines also a large, prospective trial showed a significantly poorer head growth in infants with heart failure compared to placebo but no improvement of clinical symptoms, weight gain, and prognosis. Since the first reports in 1998, there are only a few long-term data available from patients with early life stress from heart failure in infancy, who are treated with beta-blockers. Our data gives cause for hope, that beta-blockers in infants with heart failure improve catch up growth and heart rate variability in long-term follow up that is clearly related to neurodevelopment and long-term cardiovascular risk.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research

Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.


