


IntelliPaper
Abstract
Introduction: The aim of this study was to establishthe correlation between urinary pathologies and anorectal malformationsand Hirschsprung's disease andpresent their therapeutic particularities.
Means and Methods: We retrospectively conducted a descriptive study at the Pediatric Surgery Department of the Queen Fabiola Children's University Hospital (HUDERF) in Brussels. We got a clearanceconsent fromthe ethical committee of our hospital. During one month, we retrieved files of children who consulted for anorectal malformations and Hirschsprung’s diseases from August 1, 2011 to June 31, 2024. We Included all patients presenting Hirschsprung’s disease and those with upper anorectal malformations. We excludedpatients who presented lower anorectal malformations. Clinical parameters that we recorded included: age, sex, type of imaging, type of urinary abnormalityand treatment.Data were analyzed with Microsoft Office Excel 2010 and SPSS 2.0 software.
Results: We included 50 patients in our study; 16 cases of upper anorectal malformations and 34 cases of Hirschsprung's disease. For radiologic assessments, 30 patients underwent abdominal ultrasound (US) and urethrocystography wasdone in 8 patients. Sevencases of urologic anomalies were associated to anorectal malformations 43.8%. The different urinary abnormalitiesfound were multicystic kidney (3 cases), vesicoureteral reflux(2 cases) and renal dysplasia (2 cases). Four cases of urologic malformations were associated toHirschsprung's diseaseat least 11.8% (2 cases of megaureter and2 cases of hydronephrosis). The conservative treatment has been practiced associated to antibiotic prophylaxis in10 cases.
Conclusion: This study is showing that urogenital abnormalitiesaremostly associated to anorectal malformations than Hirschsprung's disease. In many casesthe treatment is conservative
Explore Digital Article Text
Irène Nadine Kouna Tsala , Pierre Lingier , Tobie Eric Ntsobe , Eduardo Vieira Cardoso , Cyrille Abega , Nasroola Damry , Basile Essola & Anna Poupalou
I. INTRODUCTION
Urogenital anomalies involve morphologic and functional anomalies resulting from embryonic developmental disorders of the urinary tract and genital organs [1]. These anomalies are commonly described as genital malformations and congenital anomalies of the kidney and urinary tract (CAKUT). Genital malformations may affect the penis, scrotum, or testes in male gender, and vagina or labia in female. CAKUT affects the kidneys, ureters, bladder, and urethra. These anomalies can be isolated or syndromic [2]. When syndromic, they may be associated with Hirschsprung's disease or anorectal malformations. Hirschsprung's disease is a congenital disorder involving the intrinsic nerve plexus, which is abnormally absent from the digestive wall. Anorectal malformations are congenital conditions arising from a developmental disorder of the posterior intestine, resulting in abnormalities that affect the rectum, anal sphincter, and/or urogenital system. Anorectal malformations are classified based on the position of the rectal pouch in relation to the puborectal sling of the anal sphincter muscles. High malformations occur when the rectum does not reach the pelvic floor, while low malformations occur when the rectum extends down to the perineum.
The diagnosis of urogenital anomalies must be done during the antenatal period with obstetrical US. The appropriated treatment depends to the type of malformation and its impact to the renal function without treatment. Then, out of surgery, a conservative treatment usually gives good results. Urogenital anomalies are responsible of approximately 50% of end-stage renal disease in children [5]. It is important to make an early clinical diagnosis and provide prompt management of these anomalies to prevent progression to renal failure.
Therefore, we conducted a retrospective study that aimed to establish the correlation between urinary pathologies and anorectal malformations or Hirschsprung's disease and present their therapeutic particularities.
II. METHODS
The study was conducted at the Pediatric Surgery Department of the Queen Fabiola Children's University Hospital (HUDERF). Ethical approval was obtained from the Ethics committee of the Queen Fabiola Children's University Hospital. Patient consent was not required due to the retrospective nature of the study. We retrospectively reviewed files of patients who were admitted in our Department for anorectal malformations and Hirschsprung's disease from
August 1, 2011, to June 31, 2024. We Included all patients presenting Hirschsprung's disease and those with upper anorectal malformations. We excluded patients who presented lower anorectal malformations. Medical imaging, including abdominal US, cystourethrography (VCUG) and Magnetic Resonance Imaging (MRI), was used to diagnose and identify the type of urinary malformation.
Clinical parameters that we recorded included: age, sex, type of imaging, type of urinary abnormality, and treatment. Patient's data were stored in the X-Care system of the HUDERF. Data were analyzed with Microsoft Office Excel 2010 and SPSS software.
III. RESULTS
Demography Characteristics
Our study included 50 patients, comprising 32% (16 cases) with anorectal malformations and 68% (34 cases) with Hirschsprung's disease (Figure 1). The mean age of this sample was 15 months with the median of 5 months and the extremes ranged between 1 month and 132 months. The largest age group was between 2 and 6 months, accounting for 54% of cases (Figure 2). The sex ratio was 1 girl for 3 boys in both anorectal malformations and Hirschsprung's disease (Figure 3). In a total of 10 boys with urinary anomalies, 5 were associated to anorectal malformations and 5 others to Hirschsprung's disease. 2 girls presented urinary anomalies both associated to anorectal malformations. No urinary anomalies were observed in female patients with Hirschsprung's disease.
Imaging Finding
The abdominal US was the most imaging assessment in 30 cases and the cystourethrography (VCUG) in 8 cases. We also found 1 case of scintigraphy and 3 cases of magnetic resonance imaging (Figure 4).
Seven cases of urologic malformations were associated to anorectal malformations 43.8%. The different urinary abnormalities found were multicystic kidney (3 cases), vesicoureteral reflux (2 cases) and renal dysplasia (2 cases). 4 cases of urologic malformations were associated to Hirschsprung's disease at least 11.8%. Different malformations were megaureter (2 cases) and hydronephrosis (2 cases) (Table 1).
Treatment
The management approach was conservative in 10 cases and the surgical treatment included orchidopexy, hydrocele treatment, hypospadias repair and fistulectomy (Table 1).
IV. DISCUSSION
We conducted a single center series in a short period; and this can justify our small sample size compared to others studies .
Demography Characteristics
The predominance of male gender with 10 boys for 2 girls in urinary tract anomalies has been since described by several authors [5; 6] out of specific anomalies found in boys and not in girls, such as hypospadias and cryptorchidism.
Imaging Finding
The abdominal US focused to the urinary tract (Figure 4) was the most imaging assessment in our study and has been described by other authors as the primary diagnostic tool of the urinary malformations [1; 5; 6]. It has advantages to be a non-invasive exam without radiation exposure of the newborn baby. However, as an operator-dependent exam, sometimes, it requires an additional exploration to confirm the diagnosis. Nevertheless, US (Figure 5) plays a key role in early diagnosis of such anomalies during pregnancy and in the follow-up of those patients [2]. Cystourethrography (VCUG) was mostly performed after US (Figure 6) and remains the gold standard for diagnosing the vesicoureteral reflux as reported in other studies [1]. It was performed in one case of Hirschsprung disease, where renal cavity dilation was observed on US. This indicates that VCUG was not routinely requested in Hirschsprung's disease cases unless there were suggestive signs. In anorectal malformations, VCUG was performed in of patients. This exploration is more requested in anorectal malformation than in Hirschsprung's disease due to the higher incidence of urinary anomalies found in anorectal malformations, particularly in the digestive communication with the urinary tract described as fistula. According to Goosse et al. [5], 50% of anorectal malformations are associated to urinary anomalies. In our series we found 43.8%, this result can be similar Magnetic Resonance Imaging (MRI) was also required when ultrasound could not bring satisfaction especially to differentiate renal parenchyma (Figure 7) [1]. It was assessed in 3 patients within 2 cases of anorectal malformations and 1 case of Hirschsprung's disease. No assessment was requested in 12 cases of Hirschsprung's disease, suggesting that urinary malformations are not commonly associated to Hirschsprung's disease.
Urinary Anomalies
Congenital urinary anomalies are responsible for 50% of pediatric renal failure and mostly found in anorectal malformations. In Hirschsprung disease, urinary anomalies are rare but not absent [5]. According to Alessio Pini et al. [7], their incidence is 6-7% in Hirschsprung's disease. Our series reported 11.8% of urinary anomalies associated to Hirschsprung's disease. Many authors reported that Urinary tract anomalies are frequently associated to anorectal malformations and less associated to Hirschsprung's disease [4,5]. Furthermore, Pini Prato et al. [7] reported that, congenital urinary anomalies associated to Hirschsprung's disease are asymptomatic and therefore not routinely investigated by clinicians; then often being discovered accidentally. Other authors, such as Hoffman et al. [3], believe that the presence of urinary anomalies in Hirschsprung disease has long been underestimated, as most of these anomalies are not surgically treated. The most common urinary anomalies found in anorectal malformation were multicystic kidney, vesicoureteral reflux (VUR), and renal dysplasia. According to Sanchez et al. [4], VUR is the most frequent urinary anomaly in pediatrics, often associated with anorectal malformations and is typically manifested by urinary tract infections after the neonatal period. In Hirschsprung's disease, hydronephrosis and megaureter were urinary anomalies associated.
According to Hoffman et al. [3,8], these anomalies are commonly associated to Hirschsprung's disease, but are less diagnosed because they are usually asymptomatic.
Treatment
The Conservative treatment was commonly used combined to antibiotic prophylaxis. This choice is justified by the fact that most of these malformations are associated with urinary tract infections, which can progress to renal damage without treatment . Surgical treatment was planned for the future in case of compromised urinary function in the patient. In our series, no case was managed surgically.
V. CONCLUSIONS
Our findings confirm that urinary anomalies are more frequently associated with anorectal malformations than with Hirschsprung's disease, aligning with previous literature.. The abdominal US focused to the urinary tract is the most imaging tool used for diagnosis. While ultrasound remains the primary diagnostic tool, VCUG or MRI should be considered in cases where ultrasound findings are inconclusive or suggest complex urinary anomalies.. The treatment is either surgical in cases of compromised urinary function in the patient or conservative associated to antibiotic prophylaxis. Conservative treatment is indicated in the absence of clinical manifestations of urinary anomalies. Urinary anomalies are frequently asymptomatic in Hirschsprung's disease, which often leads to a missed diagnosis. In anorectal malformations, however, the majority of cases are associated with urinary anomalies, highlighting the importance of systematic screening for these anomalies in affected patients.
Declarations
-
No conflicts of interest were reported among the study participants.
-
Informed consent obtained by the ethics committee.
-
No funding.
-
Acknowledgements to the Medical Training Support Fund (FOSFOM) of Free University of
Brussels, Belgium, and the University of Douala, Cameroon.
Figure 5: Renal anomaly, left kidney atrophy (left) seen on ultrasound, and normal kidney on the right in the same patient
Figure 6: Cystography Showing Left Vesicoureteral Reflux (Vur) And Right Rectourethral Fistula
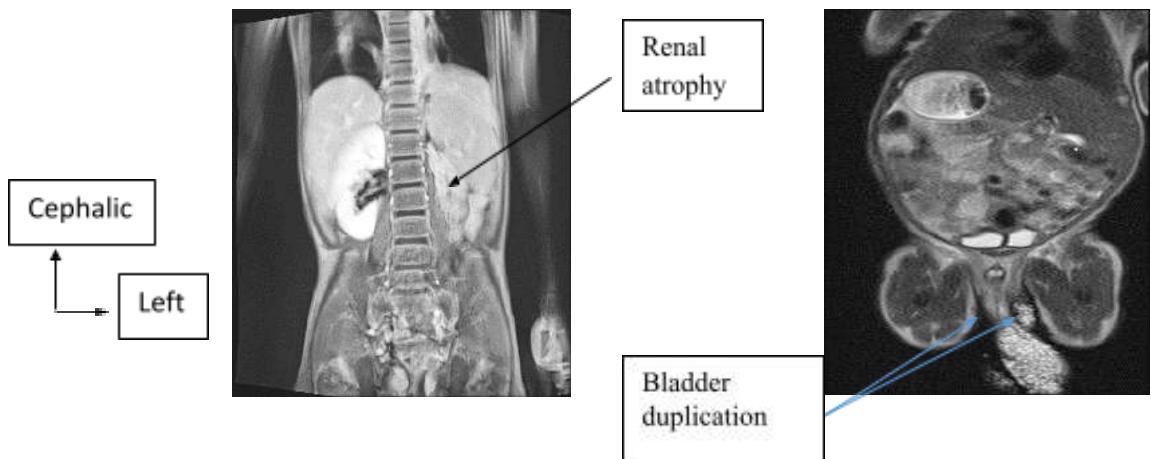
Figure 7: MRI Showing Left Renal Atrophy (At Left) And Blader Duplication (At Right)
Table 1: Distribution of Patients according to Pathology and Treatment
| Anorectal Malformation | Hirschsprung Deseas | Treatment | |
| PATHOLOGIES | |||
| VESICO-URETERAL REFLUX | 2 | 0 | Conservative + Antibiotics (ATB) |
| RENAL ATROPHY | 1 | 0 | Conservative |
| RENAL DYSPLASIA | 2 | 0 | Conservative |
| MULTICYSTIC KIDNEY | 3 | 0 | Conservative |
| MEGAURETER | 1 | 2 | Conservative + ATB |
| RECTO- URETRAL FISTULA | 1 | 0 | Fistula closure |
| HYPOSPADIAS | 0 | 1 | Uretroplasty |
| RENAL DUPLICATION | 0 | 1 | Conservative |
| HYDROCÈLE | 0 | 1 | Hydrocele repair |
| JUNCTIONAL SYNDROME | 0 | 1 | Conservative |
| HYDRONEPHROSE | 1 | 2 | Conservative |
| CRYPTORCHIDISM | 1 | 0 | Testicular descend |
| URETEROCELE | 1 | 0 | Conservative |
| SINGLE KIDNEY | 1 | 0 | Conservative |
| BLADdER DUPLICATION | 1 | 0 | / |
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research



Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.
