

IntelliPaper
Abstract
Renal cell carcinoma, (RCC) the most prevalent of kidney cancers, is a relatively common cancer, constituting approximately 10% of all cancers in adults. Many molecular subtypes have been characterized for RCC, the most common being clear cell RCC, or ccRCC, which occurs in close to 75% of cases, and has a strong association with mutations in the von Hippel-Lindau (VHL) tumor suppressor gene [1]. ccRCC constitutes close to 80% of metastatic presentations. Histology shows acinar growth and clear cell cytology, surrounded by a rich vasculature. Having a strong association with mutations in the von Hippel-Lindau tumor suppressor gene, ccRCC exhibits loss of VHL gene by 3p chromosomal loss at the 3p25 locus. Another histologic subtype includes non clear cell renal cell carcinoma nccRCC. Somatic ccRCC is characterized by inactivation of the protein products of VHL (pVHL), which promotes transcription of genes implicated in tumor formation and growth [1].
Localized and systemic therapies differ on the basis of clinical presentation such as primary or metastatic disease, and they can be administered in first-line or adjuvant settings. Before the advent of precision medicine, renal cell carcinoma was treated with non-specific immunomodulatory agent such as cytokines [2]. IL-2 and high-dose interferon-alpha (HD IFN-alpha) were considered the treatment of choice for renal cell carcinoma due to the cancer’s predisposition for lack of sensitivity to chemotherapy and hormonal therapy, however response was variable, with varying optimal effects and occurrence of toxicity. These treatments have been questioned due to data demonstrating that when these agents are administered in combination with VEGF targets, and they have shown less than ideal efficacy. Patients progressed on disease and were required to be followed up with systemic VEGFR targets in second line settings.
Explore Digital Article Text
I. INTRODUCTION
Renal cell carcinoma, (RCC) the most prevalent of kidney cancers, is a relatively common cancer, constituting approximately 10% of all cancers in adults. Many molecular subtypes have been characterized for RCC, the most common being clear cell RCC, or ccRCC, which occurs in close to 75% of cases, and has a strong association with mutations in the von Hippel-Lindau (VHL) tumor suppressor gene [1]. ccRCC constitutes close to 80% of metastatic presentations. Histology shows acinar growth and clear cell cytology, surrounded by a rich vasculature. Having a strong association with mutations in the von Hippel-Lindau tumor suppressor gene, ccRCC exhibits loss of VHL gene by 3p chromosomal loss at the 3p25 locus. Another histologic subtype includes non clear cell renal cell carcinoma nccRCC. Somatic ccRCC is characterized by inactivation of the protein products of VHL (pVHL), which promotes transcription of genes implicated in tumor formation and growth [1].
Localized and systemic therapies differ on the basis of clinical presentation such as primary or metastatic disease, and they can be administered in first-line or adjuvant settings. Before the advent of precision medicine, renal cell carcinoma was treated with non-specific immunomodulatory agent such as cytokines [2]. IL-2 and high-dose interferon-alpha (HD IFN-alpha) were considered the treatment of choice for renal cell carcinoma due to the cancer's predisposition for lack of sensitivity to chemotherapy and hormonal therapy, however response was variable, with varying optimal effects and occurrence of toxicity.
These treatments have been questioned due to data demonstrating that when these agents are administered in combination with VEGF targets, and they have shown less than ideal efficacy. Patients progressed on disease and were required to be followed up with systemic VEGFR targets in second line settings.
Prognostic factors associated with low-risk and high-risk RCC in terms of different staging systems also serve to determine appropriate therapies. Established staging systems most used in the traditional cytokine era were developed by a group at Memorial Sloan Kettering Cancer Center (MSKCC) [3]. MSKCC developed one of the most widely used prognostic systems which included parameters such as performance status less than 80%, >1.5 times the upper limit of normal of serum lactate dehydrogenase, with >10mg/dL of serum calcium, and decreased length of time for the initiation of systemic therapy after initial RCC diagnosis (<1 year) [3]. The staging system stratified patients in 3 risk categories based on the number of risk factors they possessed with poor risks having 3-5 factors, intermediate risks having 1-2 factors and no risk factors for favorable prognosis. Median overall survival (mOS) had corresponding values of 5, 14, 30 months [3].
For patients who were administered VEGFR targeted therapies (to be discussed later), the International mRCC Database Consortium (IMDC) developed a new model, which added 2 more prognostic factors: high absolute neutrophil and platelet count. According to Barata et al, "[i]n a population-based study with more than 1000 patients who received second-line targeted therapy for mRCC, the median OS was 35.3, 16.6, and 5.4 months for the favorable-risk, intermediate-risk, and poor-risk groups, respectively [3]." The lower median OS in the poor-risk groups may indicate the prognostic factors of high absolute neutrophil and platelet count would indicate lack of clinical efficacy of the VEGFR inhibitor.
There is considerable debate surrounding the use of these targeted treatments for RCC. Systemic therapies for both localized and metastatic disease present with contradictory evidence in terms of conflicting median progression free survival (mPFS), median overall survival (mOS) and overall response rates (ORR). Vascular endothelial growth factor receptor (VEGFR) antiangiogenic agents were regarded as the mainstay for treating RCC, but recent evidence suggests that they may not be as effective. Mammalian target of rapamycin (mTOR) inhibitors demonstrated efficacy in a number of clinical trials, but controversy exists over their usage in clinical settings. Clinical trials for investigational compounds have emerged, including a new class of inhibitors called HIF inhibitors and a novel drug-antibody conjugate, but some have had relatively disappointing results. Immunotherapy agents, such as immune checkpoint inhibitors (ICIs), have made substantial inroads in the treatment of clear cell mRCC and have even entered into consideration as front line settings.
Since then, other second and third generation targeted therapies have emerged to overcome resistance of these first-generation agents, (tivozanlib, axitinib, cabozantinib and vorolanib) and combination approaches have been developed to ameliorate outcomes with more favorable toxicities. This paper serves as a review of novel targeted therapies for RCC, particularly localized and advanced ccRCC, and provides additional evidence for the clinical outcomes of these targeted therapies. [1,3,4].
1.1 VEGF/VEGFR/PDGFR (Platelet Derived Growth Factor Receptor) Targets
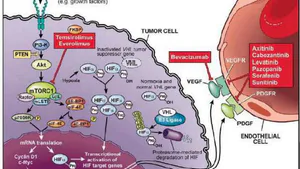
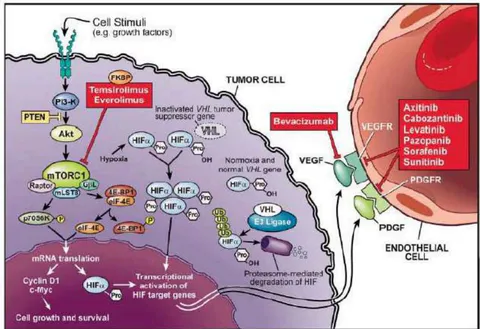
With discovery of the molecular alterations, such as the biallelic mutations inactivating the VHL tumor suppressor gene which leads to oncogenesis and ccRCC, targeted therapies such as bevacizumab, a VEFG-A targeted biologic, sunitinib, paxopanib and axitinib (the latter three being oral small molecule tyrosine kinase inhibitors that target VEGFR and PDGFR and have anti-angiogenic effects. (Figure 1) were studied in a series of clinical trials and proved to have robust clinical outcomes and favorable safety profiles that initiated a paradigm shift in the treatment of renal cell carcinoma from cytokines to targeted therapies [2]. VHL is implicated in the hypoxia-inducible pathway (HIP) which leads to overexpression of VEGFR and PDGFR, accounting for the clinical efficacy of these anti-angiogenic agents.
Bevacizumab, a biologic targeting VEGF-A, was evaluated in randomized clinical trials and compared with IFN-alpha and placebo in front-line settings. In both trials, bevacizumab demonstrated superiority in PFS: more than twofold in PFS and a PR (partial response) greater than 2 years versus placebo; a mPFS of 10.2 months versus 5.4 months and response rate of 31% versus 13% with a medium duration of greater than 1 year when compared to IFN-alpha. Both trials elicited favorable safety profiles for bevacizumab which exhibited proteinuria and hypertension that lacked severity. Both results were confirmed in subsequent trials The success of bevacizumab could be due to strength in overcoming toxicities but maybe in a limited in overcoming intrinsic and acquired drug resistance.
Concomitantly, oral small molecule tyrosine kinase inhibitors (TKI) targeting VEGFR, such as sunitinib and sorafenib, were tested in clinical trials on untreated patients and both showed superiority over IFN-alpha in phase III trials. Sunitinib showed a mPFS of 11 months versus 5 months when compared IFN-alpha with a response rate of 31%. Sorafenib was compared to placebo in patients resistant to cytokine therapy and exhibited superiority over placebo with a mPFS of 5.5 months and 2.8 months, respectively.
Common adverse events (AEs) of greater than 20% consisted of fatigue and diarrhea, which were managed with dose reduction and changes to the dosing schedule. Another TKI, pazopanib displayed superiority over placebo and non-inferiority over sunitinib in phase III trials with better quality of life and less fatigue. Overall, antiangiogenic agents were implemented in first-lines settings and displaced generalized cytokine therapies. The clinical success of antiangiogenic targeted agents such as TKIs sunitinib and sorafenib with mPFS of 11 months and 5.5 months respectively versus placebo is associated with off-target effects however. (Mabeta) One review reported that "combining FGF/FGFR inhibitors with VEGF/VEGFR inhibitors are an excellent way to optimize the curative effect and expand the antitumour range because their combination can target both tumour cells and the tumour microenvironment." However, data for RCC was not reported.
Likewise, another target implicated in the HIF pathway was mTOR which led to the development of additional medications in the treatment of clear cell renal carcinoma. The mTOR pathway also leads to angiogenesis through its interaction with the HIF pathway. These mTOR inhibitors were shown in preclinical models to have antitumor activity, such as temsirolimus and everolimus for advanced ccRCC.
A treatment-naive patient population with poor risk was administered temsirolimus and compared with IFN-alpha and had mOS of 10.9 months versus 7.3 months. 20% of patients experienced side effects, which included rash, diarrhea, anemia, hyperglycemia. The RECORD-1 phase III study for late-stage ccRCC evaluated the oral mTOR inhibitor everolimus, was compared with placebo and was shown to have improved PFS of 4.0 months versus 1.9 months [2].
1.2 mTOR Inhibitors
A randomized phase 3 trial, RECORD-1, compared the efficacy of everolimus with placebo in 410 advanced RCC patients that had prior antiangiogenic therapy (sunitinib 46%; sorafenib 28%, both agents 26%) and were non-responsive. mPFS was 4 months and 1.9 months in the mTOR inhibitor arm and placebo respectively (HR, 0.30; 95% CI, 0.22-0.40). After updated analysis, mOS were 14.8 months and 14.4 months in the treatment arm and control group, respectively (HR, 0.87; P5.162). AEs were uncommon, with 13% of patients discontinuing treatment because of them. However, stomatitis, diarrhea and fatigue did occur [3].
In the treatment of renal cell carcinoma, anti-angiogenic tyrosine kinase inhibitors and mTOR inhibitors have emerged as efficacious treatments in the first-line settings, including bevacizumab, pazopanib, sunitinib, lenvatinib, which serve as potent VEGFR TKIs, and mTOR inhibitors everolimus, and temsirolimus [5]. Another trial evaluating sunitinib compared sunitinib to interferon-alpha and the data showed longer survival, with mPFS being 11 months for sunitinib and 5 months with IFN-alpha with an hazard ratio of 0.42 (95% CI, 0.32-0.54; P <.001). [6] Another trial demonstrated pazopanib efficacy was similar to sunitinib demonstrating mPFS of 8.4 months and 9.5 months for pazopanib and sunitinib, respectively [6].
1.3 Next Generation Targeted Treatments
Cabozantinib: Meteor, Cabosun studies
A number of additional clinical trials have evaluated new targeted therapies for renal cell carcinoma in the adjuvant setting after surgical resection as single-line therapies. One of them is cabozantinib, an oral TKI targeting MET, VEGFRs and AXL.
The phase III Meteor trial comparing cabozantinib with everolimus in patients with advanced RCC and showed superior efficacy and safety in all groups evaluated: <65 (n=394), 65-74 (n=201) and >≥75 years (n = 63) [7]. Patients, who must have had prior therapy with a VEGFR TKI and exhibited 6 months of progression were deemed eligible, and were randomized 1:1 with a 60 mg once daily administration of cabozantinib and 10 mg once daily of everolimus. Cabozantinib demonstrated greater PFS with hazard ratios of 0.53, (95% CI 0.41–0.68) 0.53 (95% CI: 0.37–0.77); and 0.38 (95% CI: 0.18–0.79) for <65, 65–74 and ≥75 years, respectively. OS HRs were also observed to be significant, being 0.72 (95% CI: 0.54–0.95); 0.66 (95% CI: 0.44–0.99) and 0.57 (95% CI: 0.28–1.14). The ORRs were 15% vs 5%, 21% vs 2% and 19% vs 0% for cabozantinib versus everolimus, respectively [7]. Safety profiles were similar across all subgroups in terms of Grade III/IV AEs, with more frequent occurrences of fatigue and hypertension in the cabozantinib arm. Treatment discontinuation or dose reductions were more common in older patients, especially in the ≥75 years cohort [7].
The METEOR trial was motivated by the absence of data outcomes in patients aged 65 or greater, which although representing half of patients newly diagnosed patients with RCC, and are comprised of only a small proportion of phase III advanced RCC clinical trials. Other targeted therapies for advanced RCC patients have presented with greater efficacy, however for younger subgroups of patients.
The Meteor trial was followed by the Alliance A031203 Cabosun trial, which also evaluated cabozantinib. Cabosun compared the health-related quality of life of patients treated with cabozantinib versus sunitinib in advanced renal cell carcinoma patients who had no prior treatments . Their malignancies were considered poor or intermediate risk for enrollment and evaluation in a randomized, open-label, phase 2 trial. A total of 150 patients received treatment with either cabozantinib (n=78) or sunitinib (n=72). Males comprised 78% of the intent-to-treat population and other patient characteristics were ECOG scores of 0 (45.9%) or 1 (41.4%). Patients had either intermediate (81%) or poor-risk (19%) disease, while 36% exhibited bone metastasis .
Approximately 81% of patients had intermediate-risk. Daily dosing was 60 mg/day of cabozantinib and 50 mg/day of sunitinib in a 1:1 randomization. Treatment was discontinued upon progression of disease, therapy intolerance, or voluntary withdrawal or death [8].
Cabozantinib belongs to a class of tyrosine kinase inhibitors targeting VEFG, MET and AXL. It received prior approval in 2016 by the FDA for advanced renal cell carcinoma patients who had no previous antiangiogenic treatments. Evaluable criteria included 3 health states, time spent without toxicity before progression of disease or TWiST, time spent with toxicity before progression of disease, or TOX, and time after disease relapse or REL, progression to death. A summative measure of these durations is Q-TWiST, which is the sum of the mean time in each state. Kaplan-Meier survival curves were generated for each treatment arm and assessed for TWiST, REL and TOX by assessing the area under the curve. (Figure 2).
{"image_source":{"path":"images/243383d882c20e2ee2f419dcf13d4ab03e91180738c905d9577fd4fa932986d8.jpg"},"content":"","chart_caption":[],"chart_footnote":[]} {"image_source":{"path":"images/401ba5c3e4cbc391679ccb864d286a78df95a30a0331ea6a308f3f354a15fdc5.jpg"},"content":"","chart_caption":[{"type":"text","content":"Figure 2: Kaplan-Meier Survival Curves for cabozantinib (top) Versus Sunitinib (bottom) (adapted from Chen et al) [8]"}],"chart_footnote":[]}
According to the data revealed by the study, mean days were 317 days (cabozantinib) and 180 days (sunitinib) for TWiST with a mean days difference of 137 days and a 95% CI of 60-214. Data for TOX were 31 days (cabozantinib) and 39 (sunitinib) with a mean days difference of -8 and a 95% CI of -25 to 9. REL results were 154 (cabozantinib) and 259 (sunitinib) with a means difference in days of -105, and a 95% CI of -206 to -5 [8].
The study authors demonstrated statistical significance for Q-TWiST differences in patients with advanced RCC, which were observed to be of longer duration for cabozantinib versus sunitinib, (+ 92 (95% CI 5-178 days) and +137 (95% CI of 6-=214 days)), with a difference range of +24 days to +137 days. These results translated into positive health outcomes in terms of quantity and quality of life, with the advantage of cabozantinib conferring extended time for patients prior to cancer progression [8].
Axitinib has also emerged as a VEFGR targeted agent in the second line setting. In the AXIS study, axitinib was compared to sorafenib and PFS served as the primary endpoint. Axitinib was administered after treatment with bevacizumab plus interferon-alfa, temsirolimus, (mTOR inhibitor) or cytokine therapy. PFS was 6.7 and 4.7 months for axitinib and sorafenib respectively (p<.0001) [3].
Other novel investigational compounds were evaluated in mRCC patients, however with inconclusive results. In a randomized phase II study a novel antibody-drug conjugate called AGS-16C3F that targets a cell-surface ectonucleotide pyrophosphatase/phosphodiesterase 3 (ENPP3) conjugates to a microtubule disruptive agent: The primary endpoint of investigator-assessed PFS was not met when AGS-16C3F was compared to heavily pretreated mRCC patients with any histology and stage of disease progression [9]. Patients randomized 1:1 received the investigational compound intravenously at 1.8 mg/kg every three weeks or oral axitinib at a starting dosage of 5 mg twice daily. Out of 133 patients, 84 reached data cutoff, and the median PFS were 2.9 months and 5.7 months for AGS-16C3F and axitinib respectively (HR 1.676; 95% CI 1.107-2.537). OS was the secondary endpoint, and there was similarly no significant differences among cohorts observed. Adverse events ranged from fatigue (53%) and nausea (47%) in the AGS-16C3F cohort and similar trends (fatigue 57%; diarrhea 48%) in the axitinib arm, which were expected for both targeted therapies from previous studies. However, ocular toxicities were more common in the patients receiving AGS-163F versus axitinib (48% and 17% respectively) [9]. The study investigators concluded "[t]he investigational compound, AGS-16C3F, did not meet the primary endpoint of this trial," and further studies are not expected to be conducted in this patient population. [9] As shown, these single-line agents have met primary endpoints in clinical trials and led to antitumor activity in RCC patients, and demonstrate "modest efficacy" as monotherapies and have led to increased resistance that develop as a result of dual feedback mechanisms that inactivate the von Hippel-Landau gene, implicated in tumor aggressiveness and poor survival outcomes for RCC, particularly clear-cell RCC. Also, these small molecule TKIs, such as sunitinib, sorafenib, and pazopanib, have multiple targets and inhibit more than ten targets with non-specificity, resulting in shorter duration of therapy at the maximum tolerated dose, thus impacting the their potential as optimal therapies.
A third generation agent, tivozanib, a selective VEGFR inhibitor, was compared to sorafenib in a phase 3 trial in treatment-naïve RCC patients exhibiting metastasis. A mPFS of 11.9 months was elicited for tivozanib in comparison to sorafenib with a mPFS of 9.1 months (HR, 0.80; 95% CI, 0.63-0.99; P5.04). However, OS demonstrated longer survival in the sorafenib cohort: (29.3 vs 28.8 months; HR, 1.24; 95% CI, 0.95-1.62; P5.1.05), which led to the Food and Drug Administration (FDA) to deny approval for the tivozanib. [3]
HIF Inhibitors
Other new agents under development are a class of small molecule inhibitors that target HIF directly, which occurs upstream of angiogenesis activation. One of the first compounds studied in this category is the "first-in-class HIF-2α inhibitor PT2385" that was evaluated in a phase I trial on previously treated clear cell mRCC patients that demonstrated a favorable safety profile and a significant ORR of 14% [2]. Another agent MK-6482 in the same category as PT2385 (but constituting a second-generation agent) was evaluated in a phase I/II study in a patient population with clear cell mRCC and elicited significant ORR (24%) and mPFS (11.0 months). The efficacy of this agent was evaluated with mTOR inhibitor everolimus in previously treated mRCC patients and is undergoing investigation in a phase III study [2].
Novel investigational therapies have been developed that target rare alterations in RCC. One has been discovered and is based on the identification on several fusion partners with ALK, including VCL, TPM3, and EML. Results on the targeted therapy administration of entrectinib (RXDX-101) were reported by Tao et al [10]. Entrectinib is an agent that targets the VCL-ALK fusion, a rare mutation in RCC patients. 517 samples derived from 561 RCC patients underwent mutational profiling through broad, hybrid capture-based next-generation sequencing (NGS) using the Integrated Mutational Profiling of Actionable Cancer Targets assay and HiSEquation 2500 (Illumina, San Diego, CA) [10].
A total of three patients or 0.6% out of this cohort were found to harbor ALK fusions. One of these three patients was eligible for clinical trial enrollment investigating the efficacy of entrectinib, a targeted agent against ALK. A primary tumor was found through NGS to have a VCL-ALK translocation that generated a novel fusion gene between exon 16 of VCL and exon 20 of ALK. IHC validated the detection of ALK overexpression; FISH confirmed the fusion gene. The authors hypothesized that the existence of this VCL-ALK rearrangement in this patient would respond to first-line systemic therapy with an ALK inhibitor, such as entrectinib, and the patient was enrolled in a clinical trial of entrectinib (RXDX-101) [10]. This patient was a
22-year old male with clinical presentation of anemia and hematuria. A heterogeneous mass was detected through CT that completely replaced the right renal parenchyma. Nephrectomy was performed, revealing a RCC that exhibited pleomorphic features and metastasis of lymph nodes. Tumor resection was successful and CT confirmed no recurrence 2 months later [10].
According to Tao et al, "The patient enrolled on the 600-mg/dose escalation cohort of the phase I and IIA clinical trial of entrectinib(RXDX-101)and received entrectinib 600 mg orally per day. Response, assessed by Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, was monitored by computed tomography (CT) imaging performed at baseline, 4 weeks after treatment initiation, and approximately every 8 weeks thereafter. Treatment was administered until the patient experienced disease progression or unacceptable toxicity. Permission to publish the patient's case was obtained from his health care proxy."[10]
"Four weeks after commencing entrectinib 600 mg per day, a CT scan demonstrated a 31.4% decrease in disease, or partial response. With continued therapy, the patient attained a 61.9% decrease in disease by 15 months. The patient maintained excellent performance status throughout treatment, tolerating entrectinib well with the exception of grade 1 peripheral lower extremity edema and grade 2 weight gain. His response to entrectinib continued for 19 months, after which imaging revealed radiographic disease progression with increased mediastinal adenopathy, which led to the discontinuation of entrectinib."[10]
1.4 Combination Approaches for clear cell Renal Cell Carcinoma
Combination approaches have met with success in the RCC therapeutic area. One evaluated a potential TKI-mTOR regimen. The phase 3 trial INTORSECT compared the efficacy of sorafenib and temsirolimus in a second-line setting in 512 advanced RCC patients who progressed on sunitinib. mPFS, the primary endpoint, were 3.9 months and 4.3 months in the combination and comparator arms, respectively (HR, 1.31; 95% CI, 1.05-1.63; P5.01). [3]
Other combination regimens evaluated in clinical trials have increased options for clinicians, such as phase 2 TORAVA and phase 3 INTORACT studies evaluating bevacizumab plus temsirolimus, or bevacizumab plus sunitinib, or any mTOR inhibitor with sunitinib. These studies have shown and demonstrated superior efficacy and safety profiles. [5] A randomized combination study, CROSS-J-RCC, conducted by Tomita et al, compared sunitinib and sorafenib as front-line agents in the treatment of metastatic ccRCC. In this open-label trial, treatment-naïve metastatic clear cell renal cell carcinoma patients (n=120) with favorable or intermediate MSKCC risk were randomized to receive sunitinib followed by sorafenib or sorafenib followed by sunitinib. The primary endpoint of mPFS observed was 8.7 months and 7.0 months (HR 0.67; 95% CI 0.42-1.08) for the SU/SO and SO/SU groups, respectively [6]. Total PFS and OS served as secondary endpoints and demonstrated superiority of total PFS for the SU/SO subgroup upon analysis in patients with favorable MSKCC risk (27.8 and 22.6 months; HR, 0164; 95% CI, 0.035-0.766). However, in contrast, the HR was 11.816 (95% CI 1.355-103) in the SO/SU in patients without prior nephrectomy.
CROSS-J-RCC is particularly relevant because it included a population of intermediate risk patients who have not been closely studied prior to this study, and reflects on other prominent studies that focused on targeted agents in mRCC patients with poor prognostic factors [6].
The safety profile indicated that for the median duration of treatment for sunitinib and sorafenib was 6.7 months and 6.1 months, respectively, at data cutoff. Hand-foot syndrome, anorexia, fatigue and hypertension was seen as the most frequent AEs for sunitinib and HFS, hypertension, fatigue and stomatitis was observed as frequently occurring AEs for sorafenib. Abnormal laboratory values such as neutropenia, proteinuria and increased lipase were observed for sunitinib, while increased lipase, increased aspartate transaminase, increased alanine transaminase, and thrombocytopenia were observed with sorafenib. [6].
A new VEGFR TKI has emerged with greater efficacy at its maximum tolerated dose with less adverse events: X-82, CMo82 or vorolanib, a highly potent VEGFR/PDGFR TKI. Vorolanib is a novel kinase inhibitor that is "indolinone-based" and targets VEGFR, PDGFR and Colony Stimulating Factor 1 Receptor (CSF1R), but simultaneously exhibits low inhibition on RET and AMPK. Due to this innovative specificity, vorolanib has the potential to have a better safety profile and a large therapeutic window. In fact, in a phase 1 trial, patients tolerated this agent well at a dosage administration range from 20 to 400 mg taken daily at doses that did not reach the most tolerated dose. TRAEs ranged from nausea, fatigue, to diarrhea and vomiting in were reported in one study, while leukopenia, fatigue and hypertension were observed in another trial, however not reaching dose-limited toxicity. This led investigators to hypothesize that vorolanib when combined with mTOR target everolimus could augment antitumor activity by targeting both pathways and achieve tolerable side effect [5]. A phase I study was performed by Sheng et al. to evaluate this combination regimen and determine safety and maximum tolerated dose (MTD). Patients who had prior treatment with at least one VEGFR-TKI, such as first-line sunitinib, sorafenib, pazopanib, anlotinib and famitinib as well as second-line anlotinib, sorafenib and sunitinib were considered eligible and were administered at least one dose of the combination therapy. Table 1 shows the treatment-related adverse events; MTD was not achieved consistent with other trials in USA and China evaluating vorolanib as a monotherapy.
| Any grade, n (%) | Grade 3, n (%) | Grade 4, n (%) | |
| Proteinuria | 22 (100.0) | 1 (4.5) | 0 (0) |
| Leukopenia | 17 (77.3) | 4 (18.2) | 0 (0) |
| Hypercholesterolaemia | 17 (77.3) | 1 (4.5) | 0 (0) |
| Increased low-density lipoprotein | 15 (68.2) | 0 (0) | 0 (0) |
| Hair color change | 15 (68.2) | 0 (0) | 0 (0) |
| Hypertriglyceridaemia | 14 (63.6) | 4 (18.2) | 2 (9.1) |
| Neutropenia | 14 (63.6) | 2 (9.1) | 0 (0) |
| Raised blood glucose | 13 (59.1) | 0 (0) | 0 (0) |
| Fatigue | 12 (54.5) | 0 (0) | 0 (0) |
| Hypertension | 11 (50.0) | 4 (18.2) | 1 (4.5) |
| Creatine phosphokinase elevation | 11 (50.0) | 0 (0) | 1 (4.5) |
| AST elevation | 10 (45.5) | 0 (0) | 0 (0) |
| Diarrhea | 10 (45.5) | 1 (4.5) | 0 (0) |
| Thrombocytopenia | 9 (40.9) | 1 (4.5) | 2 (9.1) |
| Decreased hemoglobin | 9 (40.9) | 0 (0) | 0 (0) |
| Mucosal inflammation | 9 (40.9) | 1 (4.5) | 0 (0) |
| Lid edema | 8 (36.4) | 0 (0) | 0 (0) |
| Anemia | 7 (31.8) | 3 (13.6) | 0 (0) |
| Mouth ulceration | 7 (31.8) | 0 (0) | 0 (0) |
| ALT elevation | 5 (22.7) | 0 (0) | 0 (0) |
| Decreased appetite | 5 (22.7) | 1 (4.5) | 0 (0) |
| Peripheral edema | 5 (22.7) | 0 (0) | 0 (0) |
| Dyspnea | 3 (13.6) | 0 (0) | 1 (4.5) |
According to Sheng et al, "Fifteen patients had disease progression (n = 13) or death (n = 2), and the median progression-free survival was 5.6 months (95% CI: 4.6–13.0). For patients in the
1.5 Recent Clinical Trials: anti-PD-1/PD-L1 agents for ccRCC
In open-label, randomized, phase 3 CheckMate 9ER, nivolumab plus cabozantinib was shown in first line treatment versus sunitinib to have superior PFS, OS and ORR when evaluated after long-term follow-up results of 18.1 months, reporting updated safety and efficacy. The patient population was untreated and had measurable disease according to RECIST assessed by the investigator with PD-L1 testing conducted. Patients received nivolumab with cabozantinib (n=323) and sunitinib (n=328) in a random 1:1 assignment that was stratified by PD-L1 expression, among other factors. PFS by blinded independent central review was the primary endpoint and OS was the secondary endpoint. Updated mPFS was 16.6 months (12.8-19.8) versus 8.3 months ((7·0-9·7; HR 0·56 [95% CI 0·46-0·68]). mOS was 37.7 months (95% CI 35.5 to NE) in the nivolumab plus cabozantinib group versus 34.3 months in the sunitinib group (29.0 to NE) (hazard ratio [HR] 0·70 [95% CI 0·55-0·90], p=0·0043). Adverse events included hypertension (13% or 40) of 320 patients in the nivolumab and cabozantinib group and 12% or 39 of 320 in the sunitinib group and diarrhea 7%[22] versus 5%(15) in the sunitinib cohort, with grade 3-4 TRAEs in 22% or 70 of 320 patients and 10%(31) of 320 patients in the nivolumab with cabozantinib and sunitinib cohorts respectively. [13] In the phase 3, double-blind, 1:1 randomized KEYNOTE-564 trial overall survival results were reported for adjuvant pembrolizumab in ccRCC and was approved on the basis of marked disease free survival. Patients enrolled had an increased risk of recurrence and showed a significant increase according to investigator assessed DFS, the primary endpoint. OS and safety were secondary endpoints. The HR for DFS was 0.72 (95% CI, 0.59-0.87) and OS was 91.2% in the pembrolizumab cohort and 86.0% in the placebo group with benefit observed across subgroups. No deaths occurred as a result of the pembrolizumab and grade 3 or 4 adverse events were 20.7% versus 11.5%. The study showed that adjuvant pembrolizumab was associated with clinically meaningful improvement in OS. [14]
In LITESPARK-005, phase 3, multicenter, open label trial, belzutifan, a HIF 2-alpha inhibitor showed clinical activity in early phase studies when evaluated against everolimus. Of the 374 patients assigned to belzutifan in a dosage of 120 mg versus 10 mg of everolimus administered once daily, a significant part of the cohort showed improvement in PFS and OS, the primary endpoints, and the occurrence of objective response (ORR), the secondary endpoint. PFS was reported as 24% in the belzutifan group versus 8.3% in the everolimus, demonstrating cancer free of progression. ORR was 21.9% (95% confidence interval [CI], 17.8 to 26.5) versus 3.5% (95% CI, 1.9 to 5.9) in the belzutifan and everolimus cohorts respectively. mOS was 21.4 months versus 18.1 months, with 55.2% versus 50.6% of participants being alive (hazard ratio for death, 0.88; 95% CI, 0.73 to 1.07. Grade or higher side effects were higher in the everolimus group (62.5%) versus 61.8% in the belzutifan group, with treatment discontinuation occurring in 5.9% versus 14.7%, in the respective cohorts (belzutifan versus everolimus). The authors concluded that the clinical benefit of belzutifan was shown for advanced ccRCC patients who had prior therapy with immunotherapies or antiangiogenic therapies, and the treatment was associated with "no new safety signals." [15]
II. DISCUSSION
In the precision medicine era, targeted therapies for clear cell RCC have met with varied success, and while many have been shown to present with clinical activity, some outcomes of clinical trials have been modest, or even less than modest. ASSURE and S-TRAC were the first trials to evaluate sunitinib and sorafenib vs placebo presented with relatively disappointing results.
Surtime presented with data that neoadjuvant sunitinib after immediate cytonephrectomy (CN) did not have statistically significant mPFS and OS when compared to deferred CN [11]. However, when patients analyzed on an efficacy trial who progressed on IO-VEGF therapy and received a number of subsequent targeted therapies in a phase III study, Including cabozantinib, axitinib, pazopanib, lenvatinib, sunitinib, and sorafenib, post-IO-VEGF ORR was "25% and median PFS was 12.0 months (95% CI, 8.2–24.5) while the median OS was 24.5 months (95% CI, 12–NE) and 12 months OS rate was 63.3% (95% CI, 48.6–74.9) [12]."
Other complexities arise in the targeted treatment of RCC when considering the benefits of mTOR inhibitors versus VEGFR-TKI inhibitors. Evidence of the efficacy of mTOR inhibitor compared with a TKI in the first-line setting was elucidated in the phase 2 RECORD-3 trial. PFS served as the primary endpoint was reported as 7.9 months and 10.7 months for everolimus and sunitinib respectively (HR, 1.4; 95% CI, 1.2-1.8), and was not met, but did imply that TKIs had noninferiority over mTOR inhibitors, putting into question the clinical benefit of a monotherapy mTOR inhibitor such as everolimus. [3]
Further complicating the predictive analysis of RCC was evidence that everolimus actually harbored the PTEN genomic alteration rather than being involved in the mTOR pathway, a hypothesis tested in patients enrolled in the same RECORD-3 trial. Targeted NGS was employed to analyze archival specimens collected at baseline to detect mTOR pathway components, while IHC assessed PTEN expression. When everolimus-treated patients were evaluated for PTEN expression through IHCC, 50 patients who retained PTEN expression versus 50 patients who lost PTEN expression had a mPFS of 5.3 months versus 10.5 months respectively (HR, 2.5;
P < 0.001). These differences were not duplicated in the sunitinib arm (10.9 months vs. 10.3 months; HR, 0.8; P = 0.475). The investigators concluded that the "[a]ssociation between mutation status for [mTOR] and therapeutic outcome on everolimus was not confirmed.
Clinically meaningful differences in PFS were seen based on PTEN expression by IHC, lost in of patients."[16]
Additionally, in vitro assays have identified actionable targets for kidney cancer that overcome drug resistance. Porcupine (PORCN) has been shown to play a role as a palmitoyltransferase that affects the activation and secretion of the WNT pathway through transcription of Wnt proteins . Li et al found high expression of PORCN in renal cancer cell lines that have poor prognosis, and that PORCN expression occurred concomitantly with expression of Wnt proteins. LGK974, an investigational agent, was found to inhibit tumor cell growth and promote apoptosis in ccRCC cells, and prevent metastasis by reducing the expression of mesenchymal markers in a study conducted by Li et al . (Figure 3 and Figure 4).
They found that "After treatment with LGK974, the expression level of -catenin, a key protein in the classical Wnt pathway, was significantly decreased, and the expression levels of the target genes cyclin D1, c-Myc, MMP9, and MMP2 in the Wnt signaling pathway were also significantly decreased, which represented a significant decrease in the activity of the Wnt signaling pathway." Concurrently, the cell cycle of renal cancer cells was blocked significantly, and the authors concluded that "our results indicate that LGK974 could significantly inhibit the progression of renal cancer cells in a safe concentration range, so PORCN may be a safe and effective target for patients with renal cancer" [17].
{"image_source":{"path":"images/d59439186f5f11da4a57b8bcf37ebf108b5767e12ddbe4808fb8d427a08d5533.jpg"},"content":"","chart_caption":[{"type":"text","content":"(a)"}],"chart_footnote":[]} {"image_source":{"path":"images/fac2ac8fe7a0306091ed5bdeb996144e51d980ee5ffdc5ff42f5a94387e7e839.jpg"},"content":"","chart_caption":[{"type":"text","content":"(b)"}],"chart_footnote":[]}
![Figure 3: Relative miRNA Expression as an Indicator of Survival Probability (adapted from Li et al) [15]](https://doc.journalspress.com/qdbh22_108405/ocr/images/derivatives/d9/d99fb2fb7d92c92a36e7799fa43a87056ca906cc2ba6b1077a2dbe40047c98db.webp)
![Figure 4: Mesenchymal Markers in Cancerous Tissue Versus Normal Cells (adapted from Li et al) [15]](https://doc.journalspress.com/qdbh22_108405/ocr/images/derivatives/9d/9d0ed0d007f04cbffe53951561fdeee4a1a3f0af9cb1b74bc3e6bb40b8aafa1f.webp)
Finally, predictive tissue biomarkers have emerged from recent studies revealing upregulated gene signatures that predict the efficacy of treatments and open the door for liquid biopsy and circulating tumor DNA-targeted sequencing options . According to Signoretti et al in a report published in the Journal of Clinical Oncology, targets such as proangiogenic VEGF and PDGF that are implicated in the VHL-HIF pathway as a result of VHL inactivation could serve as predictive biomarkers for determining the clinical responses of VEGF-targeted therapy. These biomarkers include HIF-1a and HIF-2a and the authors cite a study by Hsieh and colleagues that "evaluated the association between somatic gene mutations and treatment outcomes in a randomized trial comparing first-line sunitinib with everolimus in patients with mRCC" . In the RECORD-3 trial, it was found that PBRM1 mutations were associated with longer PFS in the everolimus cohort, and likewise with KDM5C mutations in the sunitinib arm. It was later found in an analysis of the phase III COMPARZ trial that compared pazopanib with sunitinib in patients with locally advanced or metastatic RCC that high PBRM1 mutant tumors were associated "significantly improved OS and PFS compared with the PBRM1 nonmutant group. [1]" The authors note that this finding implicating PBRM1 alterations as a predictive biomarkers for VEGFR targeted therapy is "intriguing" since PBRM1 codes for BAF180 ("a subunit of the PBAF subtype of the switch-sucrose nonfermentable chromatin remodeling complex"), and occurs with inactivation of VHL that are both dependent on the signaling of HIF and are more sensitized to antiangiogenic agents that are "directed against the HIF target VEGF." [1]
The authors continue that "In an exploratory analysis of the IMmotion 150 trial, the expression of six angiogenesis-associated genes was identified as a potential predictive marker of response to sunitinib." In the COMPARZ trial, a different gene signature associated with the antiangiogenic agents exhibited longer PFS and OS in sunitinib or pazopanib treated patients. However, the value of PBRM1 biomarker along with the gene signatures as predictive biomarkers needs to be confirmed through further independent validation in large controlled clinical studies and future "[l]arge-scale transcriptome profiling of pretreatment ccRCC tissues has contributed to the recent identification of transcriptional signatures that might be useful in predicting clinical benefit from VEGF-targeted agents" [1].
The authors end by caveating that these analyses were conducted on patient cohorts that were limited in size, and technical issues abound in terms of experimental protocols and interobserver variability, but conclude optimistically as "larger independent and more controlled studies are needed to further clarify the significance of these findings," since "these older studies mostly relied on single-gene sequencing and single-marker immunohistochemical stains, the recent implementation of new sequencing technologies has provided a platform for large-scale biomarker discovery." [1]
III. CONCLUSION
Treatment for RCC has made significant advances from its origins in hormonal and chemotherapy through the use of immunomodulatory agents and the evolution of targeted therapy options. Targeted therapy has established itself as having robust outcomes in clinical settings evaluating VEGFR-TKIs and mTOR inhibitors and other newer third-generation and investigational agents for high-risk poor prognostic patients. While some results were modest, overall the outlook has been improved for RCC patients, especially the ccRCC molecular subtype. As recent studies have confirmed ICIs as viable therapies, future studies may explore therapies combining ICIs with VEGFR-TKIs, mTOR inhibitors and even newer agents that have shown clinical efficacy such as vorolanib and entrectinib. Clinicians can now be cautiously optimistic for treatment of patients with RCC.
Declarations Abbreviations ccRCC: Clear Cell Renal Cell Carcinoma CI: Confidence Interval CSF1B: Colony Stimulating Factor 1 Receptor CT: Computed Tomography DFS: Disease Free Survival HD IFN: alpha High-Dose Interferon-Alpha HIP: Hypoxia-Inducible Pathway ICI: Immune Checkpoint Inhibitor IL: Interleuken IMDC: International mRCC Database Consortium mPFS: Median Progression Free Survival MSKCC: Memorial Sloan Kettering Cancer Center MTD: Maximum Tolerated Dose mTOR: Mammalian Target of Rapamycin ORR: Overall Response Rate PDGFR Platelet: Derived Growth Factor Receptor PFS: Progression Free Survival RCC: Renal Cell Carcinoma SO: Sorafenib SU: Sunitinib TKI: Tyrosine Kinase Inhibitor TRAEs Treatment: Related Adverse Events VEGFR: Vascular Endothelial Growth Factor Receptor VHL: von Hippel-Landau Ethics Approval and Consent to Participate Not Applicable Consent for Publication Not Applicable Availability of Data and Material Not Applicable Competing Interests The author has stock ownership in Novartis, Merck, Eli Lilly and Bristol-Myers Squibb. Funding Not Applicable
ACKNOWLEDGEMENTS
Not applicable.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research


Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.