




IntelliPaper
Abstract
Intramedullary nails are widely used to treat extracapsular femoral neck fractures, providing a minimally invasive approach that allows early weight-bearing. However, in about 5% of cases, proper fixation is not achieved. One rare complication is the intrapelvic migration of the cephalic screw, which occurs in less than 0.5% of cases. This study reports two cases of intrapelvic screw migration and reviews the literature on this complication.
A retrospective descriptive study was conducted at our hospital between 2015 and 2022, analyzing two cases of cephalic screw migration following hip fracture treatment. Case 1 involved an 85-year-old male who underwent treatment for a right pertrochanteric fracture with a Gamma 3 nail. Three months post-surgery, the cephalic screw migrated into the pelvic cavity, requiring removal via laparotomy. A partial hip prosthesis was implanted in a subsequent surgery, and the patient recovered successfully. Case 2 involved an 83-year-old female with multiple comorbidities. After a right pertrochanteric fracture was treated with a PFNA nail, the cephalic screw migrated intrapelvically 20 months post-surgery. Due to her comorbidities, the screw was removed through the hip approach, and the patient passed away six months later from pre-existing health issues.
A literature review of 17 reported cases revealed that screw migration often occurs due to improper screw placement, repeated axial loading, and unstable fixation. Prevention strategies emphasize achieving an anatomical reduction, selecting an appropriately sized screw, and proper follow-up to detect complications early. Treatment options include screw removal via open surgery, laparotomy, laparoscopy, or endovascular approaches.
In conclusion, medial migration of the lag screw is rare but significant. Preventing this complication requires optimal fracture reduction, precise screw placement, and proper follow-up to avoid severe consequences for the patient.
Explore Digital Article Text
I. INTRODUCTION
Hip fractures are common in the elderly population, accounting for approximately 50% of fragility fractures, with their incidence progressively increasing due to population aging (1,2).
The intramedullary nail is a widely used device in trauma surgery for the treatment of extracapsular femoral neck fractures, as it is minimally invasive and allows for early weight-bearing in frail patients. However, in approximately 5% of cases, the intramedullary nail fails to achieve proper fixation in these fractures (3).
One potential complication in these fractures is cut-in, which can be classified as either early or late cut-in, depending on the stage at which it occurs. A much rarer complication is the migration of the cephalic screw into the pelvic cavity following fracture fixation, occurring in less than 0.5% of cases (4). Due to its rarity, few cases have been reported in the literature, although the complications can be severe given the anatomical location of the screw (5).
The objective of this study is to analyze two cases of intrapelvic migration, assess treatment strategies and long-term complications, and conduct a literature review of previously reported cases.
II. MATERIALS AND METHODS
A retrospective descriptive study was conducted between 2015 and 2022 at our hospital, analyzing cases of cut-in with intrapelvic screw migration as a complication of hip fracture. Two cases of intrapelvic screw migration were identified. Demographic, clinical, and radiological data were collected, along with information on complications observed in outpatient follow-ups. Additionally, a literature review of previously reported cases was performed.
Case 1:
An 85-year-old male presented with a right pertrochanteric hip fracture classified as AO type 31 A 13 (Figure 1) following a low-energy fall. The patient was admitted and underwent surgery the following day, consisting of closed reduction and implantation of a short intramedullary nail (Stryker, Michigan, United States) using a Gamma 3 nail (Figure 2). The cephalic screw was inserted into the subchondral bone in a centre-inferior position.

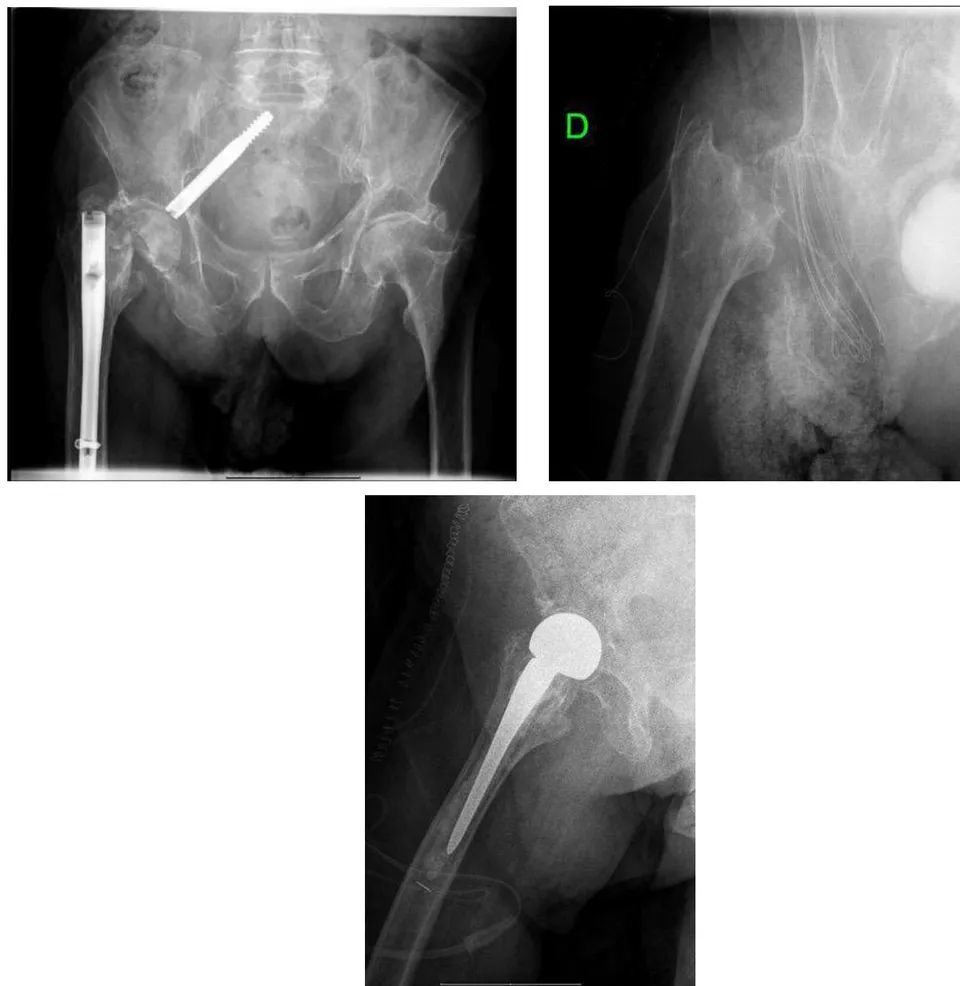
The postoperative course was uneventful; however, at the three-month follow-up, radiographic evaluation revealed cephalic screw migration into the pelvic cavity. The patient had reported a one-week history of progressive groin pain without prior trauma. Radiographic imaging (Figure 3) demonstrated intrapelvic migration of the screw through the medial wall of the acetabulum. A contrast-enhanced CT scan ruled out damage to intrapelvic organs. The screw was found positioned between the bladder and intestines, necessitating surgical removal in collaboration with the general surgery team via open laparotomy.
Following recovery from the initial procedure, a postoperative control radiograph was obtained (Figure 4). In a subsequent surgery, a cemented partial hip prosthesis was implanted (Figure 5). No bone grafting was required for acetabular reconstruction, as the bone defect was minimal.
The patient recovered successfully from the second surgery, without complications during the two-year follow-up, and was able to ambulate without the need for assistive devices.

Case 2:
An 83-year-old female with a history of congestive heart failure and poorly controlled diabetes presented to the emergency department with right lower limb pain and functional impairment following a low-energy fall. Radiographs (Figure 6) revealed a right pertrochanteric hip fracture classified as AO type 31 A 13. The patient underwent closed reduction and implantation of a
PFNA nail with a cephalic screw placed in a centre-centre position (Synthes, United States) the following day (Figure 7).
The postoperative course was complicated due to the patient's multiple pre-existing comorbidities. At 20 months, after another low-energy fall, radiographs showed intrapelvic migration of the cephalic screw (cut-in) (Figure 8). The patient had reported isolated groin pain for several months but, due to her comorbidities, had not resumed ambulation and was wheelchair-bound, delaying her medical consultation.
Given the high surgical risk and the fact that she had not ambulated since the initial surgery, the medical team opted for cephalic screw removal while leaving the intramedullary nail in place (Figure 9). This decision was made after an abdominal CT scan ruled out associated complications.
The patient's initial postoperative course was uneventful; however, she ultimately passed away six months later due to her pre-existing comorbidities.

Approach for Nail Removal N Cases Position of the Screw Time from First Surgery until Migration Laparoscopic Kuroshima et al (1 case) (6) Anterior 44 weeks Open Femoral Approach Kim et al (1 case) (7) Centre - Centre 3 weeks Anterior-medial 2 weeks Lee et al (1 case) (8) Posterosuperior 8 weeks Akçay et al (1 case) (9) - Medial - 20 weeks - Centre - 6 weeks Georgiannos (2 case) (10) - Centre Nagura et al (1 case) (11) Centre -Posterior 20 weeks Lozano-Álvarez et al (1 case) (12) Centre -Inferior 16 weeks Flint et al (1 case) (13) Centre - Centre 28 weeks Lal et al (1 case) (14) Inferior 12 weeks Heineman (1 case) (15) Inferior 3 weeks Pinheiro et al (1 case) (16) Centre - Centre 4 weeks Dragan et al (1 case) (17) Centre-inferior 8 weeks Intrapelvic approach Thein et al (1 case) (18) Antero-superior 5 weeks Robinson SJ et al (1 case) (19) Superior 44 weeks Endovascular approach Mousati et al (1 case) (5) * 4 weeks
III. DISCUSSION
Intrapelvic migration of the cephalic screw is a rare complication, with few cases reported in the literature. Among these (Table 1), the study by Rebuzzi et al. (4) highlighted that while medial migration is rare (<0.5%), it is relatively common (43%) when the screw position is considered high-risk. Regarding prevention strategies to avoid biomechanical implant failure, Georgiannos et al. (10) emphasized that achieving an anatomical reduction is key. Additionally, the appropriate cephalic screw size must be selected, maintaining a tip-apex distance (TAD) of <25 mm. Ideally, the screw should be positioned centrally or inferiorly on radiographs, and proper follow-up is essential to detect complications early.
In many cases, inadequate fracture reduction and improper screw placement, combined with repeated axial loading on an unstable fixation, can lead to displacement of the nail within the femoral canal, producing an effect similar to the "Z-effect."
A similar mechanism was proposed by Weil et al. (20) in their biomechanical study. Some studies have found no significant differences in the need for revision surgery between patients treated with the Gamma 3 nail or the PFNA nail, suggesting that screw placement may be more critical in preventing migration than the implant type itself (21).
Flint et al. (13) analyzed risk factors associated with screw penetration and medial migration, categorizing them into different groups: 1 intraoperative factors related to the surgeon, such as excessive reaming of the femoral head; 2 intraoperative fracture characteristics; 3 implant-related factors, such as screw dysfunction; 4 technical errors, including excessive TAD; and 5 postoperative factors, such as additional trauma. In our cases, the primary reason for failure in the first patient was cephalic screw placement, while in the second case, it was postoperative trauma following a fall.
A detailed clinical history and serial radiographs can aid in the early detection of this complication. In most cases, removal is performed through the previous incision; however, in some instances, due to the intra-abdominal location of the screw, extraction requires open laparotomy or laparoscopy (6), though the risk of injury to major arteries and vital organs remains present. There are also reports of successful cephalic screw removal via an endovascular approach (5). In such cases, a multidisciplinary approach is necessary to safely extract osteosynthesis material while minimizing complications, considering both screw location and the patient's comorbidities. In our two cases, one required open laparotomy in collaboration with general surgeons due to the screw's location, while in the second case, removal was possible through the previous hip approach.
Therefore, optimal fracture reduction and proper screw placement are the most crucial steps in reducing the risk of medial migration of the cephalic screw. However, continued follow-up is essential, as the increasing incidence of hip fractures may lead to a rise in this complication, which, despite its rarity, can have severe consequences for the patient.
IV. CONCLUSIONS
Medial migration of the lag screw is an uncommon but significant complication. Its prevention requires optimal fracture reduction and precise screw placement.
Ensuring correct screw insertion is crucial to avoid undesirable displacement. The biomechanics of intramedullary screws facilitate lateral screw sliding; however, in cases of unstable fixation, medial migration may occur.
Conflict of Interest
The authors declare no conflict of interest.
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research


Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.

