


IntelliPaper
Abstract
Background: Mortality trends in Emergency departments serve as vital indicators of healthcare quality and system effectiveness. Understanding the mortality patterns in these settings is crucial for optimising emergency care delivery. However, limited research exists on mortality trends in emergency departments, particularly in low-resource settings such as Ghana. This study seeks to provide valuable insights into the factors contributing to mortality and inform strategies for improving emergency care.This study aimed to analyse mortality trends in the Emergency Department of Korle-Bu Teaching Hospital in Ghana over a specified period.
Methodology: This retrospective study utilised data obtained from medical records of patients who presented to the emergency department of Korle-Bu Teaching Hospital and subsequently died during their hospital stay for the year 2023. Data on patient demographics, admission records, clinical characteristics, and diagnosiswere collected, analysed, and summarised using descriptive statistics.
Results: During the review period, the total attendance at the KBTH Accident and Emergency Centre was 14,472, comprising 8,666 males and 5,806 females. Among these attendees, 5,856 individuals were admitted. The centre reported 492 cases of Brought-in-Dead (Dead on Arrival). The age group with the highest attendance was 15-44 years. A total of 909 deaths occurred in the emergency department, with 465 males and 444 females. The age distribution of fatalitiesshowed the majority occurring in the 60+ age group. The overall mortality rate per attendance was 6.3%.The leading cause of death was cerebrovascular accident (CVA), followed by chronic renal disease and all types of pneumonia.
Conclusion: The review of mortality patterns offers valuable insights into the epidemiology, outcomes, and challenges associated with emergency care. These findings underscore the importance of ongoing surveillance, quality improvement initiatives, and interdisciplinary collaboration to enhance patient care and inform health promotion strategies in communities aimed at reducing mortality.
Explore Digital Article Text
I. INTRODUCTION
The Emergency Department (ED) is the primary gateway to any hospital and is critical in providing immediate medical care to patients with acute injuries and illnesses (1)(2)(3). Emergency care encompasses medical decision-making and the skills or competencies required to avert unnecessary mortality or disability (4). These competencies involve swiftly assessing, resuscitating, and stabilizing patients facing life-or limb-threatening conditions (4).
Mortality trends within Emergency departments serve as important indicators of the quality of emergency healthcare services and can help identify areas for improvement. Mortality rate and its associated spectrum are key health indicators requiring regular assessment in any healthcare facility (1). The emergency department serves as a vital hub for treating patients with diverse medical and surgical conditions of varying severity, facilitating interventions to correct physiological abnormalities and mitigate the progression of organ failure, thereby reducing mortality rates (3).
Conducting mortality audits in the emergency department is particularly crucial as it sheds light on various aspects, including the range of emergency cases prevalent in the community, the burden of morbidity, the demographic distribution, the efficacy of the emergency department's response, and the mortality load (1). Additionally, the profile of cases observed in the emergency department is reflective of the prevalent risk factors and disease patterns within the community (5).
Ghana, like many other low- and middle-income countries, faces unique challenges in delivering emergency medical care due to resource constraints, lack of an efficient prehospital care and transport system, severity of illness or injury, and limited access to specialized services all contributing to increase in in-hospital mortality (3). Despite efforts to strengthen healthcare systems, gaps in emergency care provision persist, contributing to adverse outcomes, including high mortality rates in emergency departments (6). The lack of comprehensive data on mortality trends and associated factors in Ghanaian Emergency departments hinders the development and implementation of targeted interventions to address this issue. Therefore, investigating hospital mortality trends is crucial for understanding the local context and informing evidence-based strategies to enhance emergency medical services. This study explores mortality trends in the Accident and Emergency Department of Korle Bu Teaching Hospital, Ghana's largest referral centre, which serves the southern region and receives a high volume of patients.
II. MATERIALS AND METHODS
This was a retrospective review of the digital data records of all patients who presented to the accident and emergency centre from 1 January
2023 to 31 December 2023 to receive care. The mortality data was collected over one year to provide a focused snapshot of the patterns and trends within a defined and recent timeframe. All patients who presented to the Accident and Emergency Centre to seek care over the specified period and died during their hospital stay were included. Ethical approval was sought from the Korle Bu Scientific Technical Committee and Institutional Review Board for the study (KBTH-IRB 00077/2024).
The Korle Bu Teaching Hospital is Ghana's largest and leading referral centre. With a bed capacity of 2000, it primarily serves the southern part of the country as a major referral hospital. It comprises 17 clinical and diagnostic departments, including the Accident and Emergency Centre, which functions as the receiving point for trauma, medical, and surgical emergencies.
The Accident and Emergency Centre comprises a triage area and three main wards (Red, Orange, and Yellow), categorised by illness acuity using the South African Triage Scale (SATS). Based on their Triage Early Warning Scores (TEWS), patients are colour-coded: Red (TEWS >6) for life-threatening emergencies, Orange (TEWS 5-6) for very urgent cases, and Yellow (TEWS 3-4) for urgent cases, while Green (non-urgent) cases (TEWS 1-2) are directed to the Korle-Bu Polyclinic. Red, Orange, and Yellow patients are admitted into the respective wards, managed by emergency medical officers and residents under specialist supervision, and referred to relevant specialties for continued care. The Clinical Decision Unit (CDU) serves as an overflow ward for the emergency department.
Records of all deceased patients who died whilst on admission at the Accident and Emergency were retrieved and organized by month. Data was extracted from the patient's electronic record system (Lightwave Health Information Systems (LHIMS)). This is the hospital's digital health platform for patients' data and clinical records.
For patients with incomplete electronic records, data were manually reconciled using ward admission and discharge registers maintained by ward nurses. All patients who died in the emergency department during the specified period were included in the analysis.
The variables collected included age, sex, clinical diagnosis (primary working diagnosis), duration of stay (in hours), and possible cause of death based on the primary clinical or working diagnosis in patient's records. Patients brought in Dead (BID) or dead-on arrival were included. Data obtained was entered into a Microsoft Excel data capture sheet, organized by months of the year, and then cleaned. Descriptive statistics were used to calculate the total number of admissions and deaths, with the results presented as frequencies and percentages in tabular form.
III. RESULTS
During the review period, the total attendance at the KBTH Accident and Emergency Centre was 14,472, comprising 8,666 males and 5,806 females, resulting in a male-to-female ratio of 1.5:1. Among these attendees, 5,856 individuals were admitted and an additional 1,456 were detained. The centre reported 492 cases of Brought in Dead (Dead on Arrival), yielding an incidence rate of 3.4%. The age group with the highest attendance was 15-44 years, with a mean age of 42.16 (Table 1).
A total of 909 deaths occurred in the emergency department, with 465 males and 444 females (Figure 1). The highest number of deaths occurred in January, followed by December. The age distribution of deaths is detailed in Table 1, with the majority occurring in the 60+ age group. The mean age was 52.66. The overall mortality rate per attendance was 6.3%.
Of the 5,856 admitted patients, 1,866 were admitted to the red ward, 1,928 to the orange ward, 1,641 to the yellow ward, and 424 to the Clinical Decision Unit (CDU). Table 2 presents the distribution of deaths per ward, with the red ward accounting for the highest fatalities (65.79%). The mortality rate per admission was 15.52%.
occurred more than 48 hours after admission (Table 3).
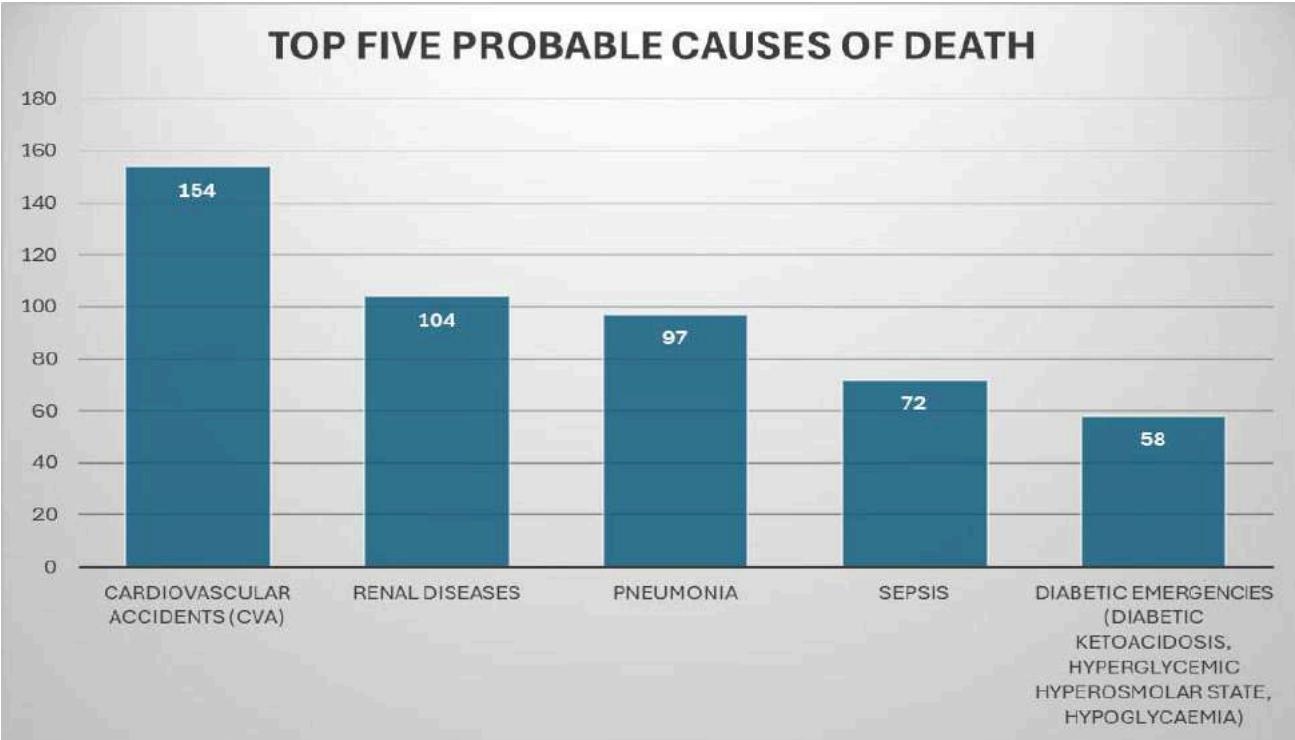
The possible causes of death based on the working clinical diagnoses are listed in Figure 3. The leading possible cause of death was cerebrovascular accident (CVA), followed by chronic renal disease and pneumonia. The leading possible cause of death within the first 24 hours was CVA, followed by Pneumonia (Table 4).
IV. DISCUSSION
The mortality patterns in Korle Bu Teaching Hospital's Emergency Department over one year provide valuable insights into the epidemiology and outcomes of patients presenting to the emergency department (ED). The findings highlight important demographic characteristics, mortality rates, ward distribution, and leading causes of death within the studied population.
The study period encompassed a total attendance of 14,472 individuals at the KBTH Accident and Emergency Centre, with a male-to-female ratio of 1.5:1. This observation aligns with existing literature indicating a higher prevalence of emergency department visits among males compared to females (7)(8)(9). Men are more prone to injuries, making them more likely to present to the emergency department.
The incidence rate of Brought in Dead patients among patient attendance was 3.4% higher than in settings with well-established pre-hospital emergency care systems (10). Although there is no standard definition of brought-in-dead, the broad definition may encompass patients who are either pronounced dead upon arrival at an emergency department without any resuscitation attempt or those who passed away after unsuccessful resuscitation efforts, typically within the first 15 to 60 minutes of arrival (10). In high-income settings with well-established prehospital settings, the BID rate is less than 2% (8). Although our BID rate did not differ so much from established settings, studies of high BID rates in other low-resource settings have been reported.
The study's findings highlight a significant aspect: the noticeable mortality rate observed within the emergency department. A total of 909 deaths were recorded, with a mortality rate of 6.3% per attendance. Morbidity and mortality rates within the emergency department of any hospital serve as indicators of the adequacy, or lack thereof, of clinical care and infrastructure (11). This underscores the critical nature of conditions managed within the ED and emphasizes the need for prompt and effective interventions to mitigate adverse outcomes. The mortality rates observed were similar to those of other studies. Okoroiwu et al recorded a mortality rate of 4.5% (12).
The age distribution of deaths reveals a higher prevalence among individuals aged 60 years and above, reflecting the increased vulnerability of older adults to acute emergencies. This was a similar finding by Okoroiwu et al (12). Research indicates that the incidence of cardiovascular diseases rises sharply with age, placing older individuals at a higher risk of mortality (13). Additionally, more men died than women, which was similar to other studies (2)(12)(14). In general, females have been found to exhibit lower mortality rates and longer life expectancies compared to males, with males having higher mortality rates from injuries in regions like Africa, Latin America, the Caribbean and Europe (12)(9). Moreover, it has been found that there is a higher prevalence of cardiovascular diseases in men than in women, putting them at higher risks of mortality (15).
In this study, the 15-44 age group had the highest attendance yet reported the third-highest number of deaths. This age group, although more active and exposed to various risk factors, may be more prone to trauma-related injuries, contributing to their high attendance. Additionally, their tendency towards seeking prompt medical care when faced with serious conditions may lead to increased ED visits. Despite high attendance and proactive health-seeking behaviours, the nature of their injuries or conditions, which could be severe or complex, likely contributed to the significant mortality observed in this group.
Analysis of mortality patterns across different months highlights notable variations, with the highest number of deaths occurring in January, followed by December. While seasonal trends in mortality have been documented in various settings, further exploration is warranted to elucidate potential contributing factors, such as climatic variations, infectious disease outbreaks, non-adherence to medications during holiday seasons or holiday-related accidents.
Ward distribution of admissions provides valuable insights into resource utilisation and patient flow within the emergency department. The red ward, which typically accommodates patients with critical or life-threatening conditions, recorded the highest proportion of deaths (65.79%). This underscores the importance of appropriate triage and allocation of resources to optimise patient outcomes, particularly for those with high-acuity presentations.
The leading causes of death identified in the study further highlight the diverse spectrum of medical conditions encountered in the emergency department. Cerebrovascular accidents (CVAs) emerged as the primary cause of mortality, followed by renal diseases and pneumonia. Recent studies strongly indicate that noninfectious diseases are increasingly recognised as significant causes of morbidity and mortality (14). In low- and middle-income countries, it is estimated that over 80% of deaths result from noncommunicable diseases (14). In a study conducted by Ugare et al., the majority of mortalities were attributed to medical causes, with a significant proportion related to terminal cardiovascular diseases (11). This highlights the critical need for early intervention and effective management of chronic and acute cardiovascular conditions to reduce mortality rates in hospital settings. Patient education, community intervention, and health promotion activities targeting non-communicable diseases, particularly cardiovascular diseases, are essential. By increasing public awareness and encouraging healthier lifestyles, we can potentially reduce the burden of these conditions and improve overall patient outcomes.
A significant portion of the deaths, 39.39%, occurred within the first 24 hours of admission and increased to 61.1% up to 48 hours of admission, highlighting the critical nature of early intervention in emergency settings. This was similar to the findings in Ugare et al study, where 56% of deaths occurred up to 48 hours after admission (11). Potential reasons attributed to these identified deficiencies within the healthcare system include delays in resuscitation and interventions and inadequate monitoring systems (11). Delays in initiating life-saving procedures and interventions can contribute to increased mortality, whilst poor monitoring systems may fail to promptly identify deterioration in a patient's condition, further increasing the risk of adverse outcomes. Addressing these inadequacies is crucial for optimising patient care and reducing mortality rates.
The leading cause of death within this period was cerebrovascular accident (CVA), followed by various types of pneumonia. These findings emphasize the importance of timely and accurate initial assessments and rapid initiation of treatment protocols to improve patient outcomes. The second-highest number of deaths, accounting for 37.51%, occurred more than 48 hours after admission. This suggests that while initial interventions may stabilize patients, a substantial mortality risk remains during the subsequent hospital stay. These findings indicate the need for ongoing, vigilant monitoring and comprehensive management strategies tailored to address the underlying pathophysiology of common acute conditions encountered in the emergency setting beyond the initial 24-hour period, particularly for chronic conditions.
V. LIMITATIONS OF THE STUDY
This study was based on a retrospective review of medical records, which posed limitations in data quality and completeness. Some records were missing, incomplete, or inconsistently documented; however, these gaps were addressed by cross-referencing ward admission and discharge registers maintained by nursing staff. The findings were based on data from a single institution, Korle-Bu Teaching Hospital, which limits the generalizability of the results to other emergency departments within the country in different settings. Variations in healthcare practices, resource availability, and patient demographics can influence mortality trends and outcomes in other locations. The study may be subjected to selection bias as it only included patients who were admitted to the emergency department and subsequently died. This cannot fully represent all cases of in-hospital mortality, as it excludes those outside the emergency department in different wards. Additionally, there could have been reporting bias in the recording of the cause of death, which may have had an impact on the outcome as the study relied solely on the primary working diagnosis as probable cause of death as reported and documented by the doctors who managed the cases.
VI. CONCLUSION
In conclusion, the review of mortality patterns in the Emergency Department of Korle Bu Teaching Hospital offers valuable insights into the epidemiology, outcomes, and challenges associated with emergency care delivery. These findings underscore the importance of ongoing surveillance, quality improvement initiatives, and interdisciplinary collaboration to enhance patient care and optimize outcomes within the emergency setting.
ACKNOWLEDGEMENTS
We acknowledge the support of the Accident and Emergency Centre staff of the Korle Bu Teaching Hospital, Accra, Ghana. The abstract of this paper was submitted for presentation at the African Conference on Emergency Medicine 2024, held in Botswana.
Conflict of Interest
The authors declare no conflict of interest.
Funding
No funding was received.
Contributions of Authors
Concept and Design: Nana Serwaa Quao, Janet Opare, Malwine Abena Obuobisah.
Acquisition, analysis, and interpretation of data: Nana Serwaa Agyeman Quao, Janet Naki
Opare, Theophilus Kpakpo Addo, Alberta Ampomah, Anthony Kofi Sakyi Amoah, Queenster Thompson, Malwine Abena Obuobisah.
Drafting of the Manuscript: Nana Serwaa Agyeman Quao, Janet Naki Opare, Theophilus Kpakpo Addo, Alberta Ampomah, Anthony Kofi Sakyi Amoah, Queenster Thompson, Malwine Abena Obuobisah.
Final review of the Manuscript: Nana Serwaa Agyeman Quao, Janet Naki Opare, Theophilus Kpakpo Addo, Alberta Ampomah, Anthony Kofi Sakyi Amoah, Queenster Thompson, Malwine Abena Obuobisah.
- deaths (39.39%) occurred within the first 24 hours, increasing to 568 (61.1%) up to 48 hours after admission. Additionally, 341 (37.51%) (p.4) ↩
Conflict of Interest
The authors declare no conflict of interest.
Ethical Approval
Not applicable
Data Availability
The datasets used in this study are openly available at [repository link] and the source code is available on GitHub at [GitHub link].
Funding
This work did not receive any external funding.
References
Cite this article
Related Research



Special Issue
Launch a focused special issue to highlight research, emerging trends, and expert insights in your academic field.
